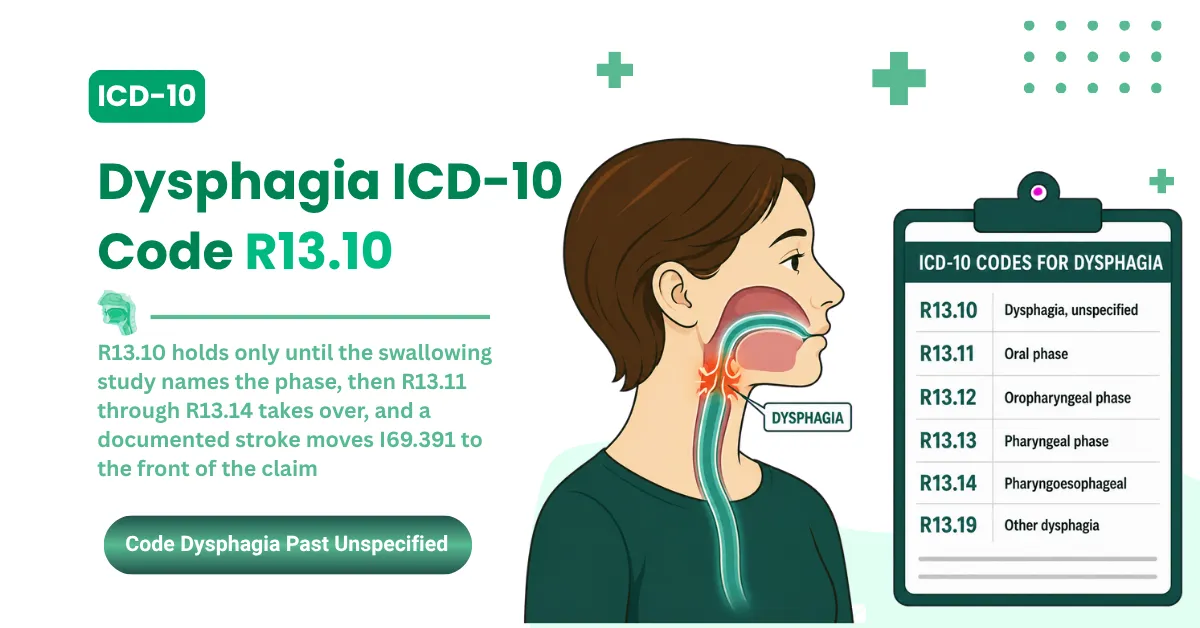


The ICD-10-CM code for knee pain is M25.561 for the right knee, M25.562 for the left knee, and M25.569 for an unspecified knee. M25.56 is the non-billable parent code, so coders pick a laterality-specific child code on every claim.
That laterality choice isn't a clerical detail. Wrong-side codes and unspecified overuse are denial generators, and payers now catch both with automated edits.
Bilateral knee pain has its own rule worth flagging up front: both codes, one claim, no combined code exists. The full breakdown is below.
This guide covers laterality, the bilateral two-code rule, the unspecified-code audit risk, the switch to M17 and S83 once a diagnosis lands, chronic pain sequencing with G89.29, and the documentation that keeps these claims clean.
What Is the ICD-10 Code for Knee Pain?
Knee pain falls under M25.56 (pain in knee) in the ICD-10-CM musculoskeletal chapter, with three billable child codes: M25.561 for the right knee, M25.562 for the left knee, and M25.569 for an unspecified knee. Bilateral knee pain requires both M25.561 and M25.562.
The parent code is where claims go wrong. M25.56 sits under category M25 in Chapter 13, and it isn't billable on its own because it's missing the sixth character that carries laterality. Submit the four-character parent and the claim trips a specificity edit before a payer reviews it.
Here's the family laid out:
- M25.561: Pain in right knee. Use when the record documents right-sided knee pain and no underlying diagnosis is confirmed.
- M25.562: Pain in left knee. Use when the record documents left-sided knee pain and no underlying diagnosis is confirmed.
- M25.569: Pain in unspecified knee. Use only when laterality isn't documented anywhere in the record.
- Bilateral knee pain: Report M25.561 and M25.562 together. No single bilateral knee pain code exists.
The specificity standard behind all of this comes from the Official Guidelines, Section I.B.2 (Level of Detail in Coding), which directs coders to the highest level of detail the documentation supports. For knee pain, that means the side, every time it's charted.
The musculoskeletal symptom-code family shares this same structure, walked through in MedSole's back pain ICD-10 guide, and the broader code-system context is in the ICD-10 vs ICD-11 guide. The full FY2026 rule set lives in the April 1, 2026 Official Guidelines PDF.
M25.561: ICD-10 Code for Right Knee Pain
M25.561 is the ICD-10-CM code for pain in the right knee. It's a billable symptom code for both acute and chronic right knee pain, used when no underlying diagnosis like osteoarthritis or a meniscus tear has been confirmed by the provider.
One thing surprises people new to the M25.56 family: there's no separate acute code. M25.561 covers a right knee that started hurting yesterday and one that's ached for a year. Duration doesn't change the symptom code. What changes it is a confirmed cause or a documented injury.
That injury distinction matters for the claim. When the note documents a mechanism, a fall, a twist, an impact, the coding moves off M25.561 to the S83 or S80 family instead. Those injury codes carry a required seventh character and tell a different story to the payer.
Injury Mechanism Check: Acute right knee pain codes as M25.561 only when no injury mechanism is documented. A documented fall, twist, or impact moves the claim to the S83 family with the required seventh character.
Documentation drives the rest. The side has to appear in the note, and M25.561 pairs with whatever E/M or therapy CPT carries the visit. Once a structural diagnosis is confirmed, M25.561 retires in favor of the specific code, and the full switch logic is in the osteoarthritis and injury section below.
The therapy CPT pairings that ride with knee pain claims are covered in MedSole's physical therapy CPT codes guide, and the full M25.561 detail sits at icd10data.
M25.562: ICD-10 Code for Left Knee Pain
M25.562 is the ICD-10-CM code for pain in the left knee. It's a billable diagnosis code used when a patient presents with left knee pain and the provider hasn't established a definitive cause such as osteoarthritis, a ligament injury, or a meniscus tear.
The left code works exactly like its right-side twin. It covers acute and chronic left knee presentations, it needs laterality documented in the note, and it pairs with the E/M or therapy CPT for the visit. When a structural diagnosis is confirmed, M25.562 steps aside for the specific code.
Here's the error that costs left-knee claims the most: defaulting to M25.569 when the chart says left. It happens when a coder grabs the unspecified code out of habit, even though the documentation names the side. That single shortcut creates the specificity problem the next section unpacks, and it's avoidable every time.
The rule is simple. If the note says left, the code is M25.562. The unspecified code is for charts that never name a side, not for charts a coder didn't read closely enough.
The full M25.562 detail sits at icd10data.
Bilateral Knee Pain ICD-10: Why You Report Two Codes
Bilateral knee pain has no single ICD-10-CM code. When a patient has pain in both knees, coders report M25.561 for the right knee and M25.562 for the left knee as two separate diagnosis codes on the same claim, because no combined bilateral knee pain code exists.
The rule comes straight from the Official Guidelines, Section I.B.13 (Laterality): "If no bilateral code is provided and the condition is bilateral, assign separate codes for both the left and right side." That's the exact language, and it settles the question that trips up so many bilateral claims.
Here's the part no competing guide explains: how the two codes sit on the CMS-1500. Both codes list in Box 21, in positions A and B, and the Box 24E diagnosis pointers link each service line to the right code. That's the mechanic that turns the two-code rule into a clean claim instead of a rejected one.
Colloquial phrasing maps to the same pair. "Left and right knee pain" and "b/l knee pain" both resolve to M25.561 plus M25.562. The words in the note don't change the coding.
Now the correction that matters most. M25.569 is not the bilateral code. Using the unspecified code for documented bilateral pain violates Section I.B.13 and Section I.B.2 together, because the side is known and the code hides it.
There's a second half to that rule, and payers enforce it with automated edits. Never report M25.569 alongside M25.561 or M25.562 on the same claim. Diagnosis-to-diagnosis edits read that combination as redundant and deny the line, the same way they catch a unilateral code billed next to a bilateral one.
Bilateral Means Both Codes: Documented pain in both knees is M25.561 plus M25.562 on one claim. M25.569 is never the bilateral answer, and it never rides alongside a laterality code.
The mechanics behind these laterality edits sit on the CMS ICD-10 codes page.
M25.569: Unspecified Knee Pain and the 2026 Audit Risk
M25.569 is the ICD-10-CM code for pain in an unspecified knee. It's billable, but use it only when the medical record doesn't document which knee is affected, because submitting M25.569 when laterality is known creates a specificity error that payers now deny automatically.
There's a narrow window where M25.569 is the right call. The side is absent from the record, the provider isn't reachable for clarification, and the claim has to go out. That's the legitimate use, and it's rarer than its billing frequency suggests.
The error is everything else. The side is charted, but the claim carries the unspecified code anyway. That's a violation of Section I.B.2's highest-specificity requirement, and it's no longer a soft compliance point. Payers run automated laterality edits that catch the mismatch on submission.
This is the enforcement shift that changed the stakes. Major national payers now deny claims that aren't coded to the laterality the record documents, through diagnosis-to-modifier and diagnosis-to-diagnosis edits that fire before a human reviews anything. The unspecified code on a chart that names the side is a denial you wrote into the claim yourself.
The audit exposure runs deeper than a single denial. A documentation-to-coding mismatch is the exact pattern that Targeted Probe and Educate review and the Office of Inspector General's improper-payment work flag in musculoskeletal claims. A habit of defaulting to M25.569 builds the pattern an auditor looks for.
Query Before You Default: If the note names the knee anywhere, the claim carries M25.561 or M25.562. M25.569 on a chart that states the side is a specificity denial you chose.
The fix is a single workflow step: query the provider for laterality before submission instead of defaulting to unspecified. MedSole RCM's coders run a laterality check on every musculoskeletal claim before it leaves the building, which is how unspecified-code denials stop recurring. See how the outsourced medical billing service works. The missing-information denials that follow these errors are broken down in the CO-16 denial code guide, and the broader compliance context sits at the OIG site.
When to Switch From Knee Pain Codes: Osteoarthritis (M17) and Injury (S83)
Knee pain codes are symptom codes. Once a provider confirms an underlying cause, the specific diagnosis replaces M25.56x. Osteoarthritis moves coding to the M17 family, and a documented injury moves it to the S83 family, per the ICD-10-CM Official Guidelines on symptom coding.
The rule has two halves, and both matter. Section I.B.4 makes symptom codes acceptable only when no definitive diagnosis is established. Section I.B.5 bars coding a symptom separately when it's integral to a confirmed diagnosis. Put together, they retire M25.56x the day the diagnosis lands on the chart.
Osteoarthritis of the knee: the M17 codes
Two documentation elements pick the osteoarthritis code: laterality, and whether the OA is primary or post-traumatic.
- M17.0: Bilateral primary osteoarthritis
- M17.11: Unilateral primary osteoarthritis, right knee
- M17.12: Unilateral primary osteoarthritis, left knee
- M17.2: Bilateral post-traumatic osteoarthritis
- M17.31: Unilateral post-traumatic osteoarthritis, right knee
- M17.32: Unilateral post-traumatic osteoarthritis, left knee
- M17.9: Osteoarthritis of knee, unspecified
When OA is confirmed, the M17 code becomes primary and the M25.56x pain code drops off the claim.
Knee injuries: when to use the S83 codes
A documented injury mechanism moves coding to the S83 family, which covers sprains, tears, and dislocations of the knee. These codes carry a required seventh character: A for the initial encounter, D for subsequent, and S for sequela. The S83 codes are what justify imaging and surgical intervention, which the symptom code can't support on its own.
|
Clinical Situation |
Code Family |
Use When |
|---|---|---|
|
Knee pain, no confirmed cause |
M25.561 / M25.562 / M25.569 |
Symptom documented, diagnosis not yet established |
|
Osteoarthritis confirmed |
M17.0 / M17.11 / M17.12 / M17.2 / M17.31 / M17.32 |
Provider documents OA with laterality and type |
|
Injury mechanism documented |
S83.x plus 7th character |
Fall, twist, or impact recorded in the note |
The April 1, 2026 release changed instructional notes only, with zero new diagnosis codes, so the M25.56x, M17, and S83 families are untouched. Undercoding after a confirmed diagnosis weakens medical necessity, which the CO-50 denial code guide breaks down. The full M17 family sits at icd10data, and the release files are on the CDC ICD-10-CM files page.
Chronic Knee Pain ICD-10: Coding G89.29 With Knee Codes
Chronic knee pain has no dedicated ICD-10-CM code. Coders report it by pairing the laterality code, M25.561 or M25.562, with G89.29 (other chronic pain) when the provider documents chronicity. Sequencing depends on whether the encounter treats the knee condition or focuses on pain management.
How to sequence G89.29 and the knee code
The order follows the purpose of the visit, per Section I.C.6. Three scenarios cover almost everything you'll see:
When the encounter treats the knee condition itself, the laterality code leads and G89.29 follows. M25.561 or M25.562 first, then G89.29.
When the visit is a dedicated pain-management encounter, that order flips. G89.29 sequences first, and the knee code comes second.
For chronic bilateral knee pain, all three codes appear: M25.561, M25.562, and G89.29, ordered by what the visit was for.
One guardrail keeps this clean. G89.29 needs documented chronicity to go on the claim at all, and it isn't added when a definitive diagnosis is being treated, unless the encounter is specifically for pain control.
Chronic bilateral and chronic left knee pain
The two laterality pairings come out as clean rules. Chronic right knee pain is M25.561 plus G89.29. Chronic left knee pain is M25.562 plus G89.29. The bilateral version runs all three, as above.
There's a sleep angle worth a note too. Chronic nocturnal knee pain that disrupts sleep can carry G47.01 when the provider documents and manages the insomnia as its own problem.
The same M25.5 joint-pain family and identical G89 sequencing show up in MedSole's left shoulder pain ICD-10 guide, the insomnia ICD-10 guide covers the G47.01 bridge, and the full M25.561 detail is at AAPC.
Associated Knee Codes: Effusion, Hemarthrosis, and Stiffness
Three code families are billed alongside knee pain when the provider documents specific findings: M25.46x for effusion, M25.06x for hemarthrosis, and M25.66x for stiffness. Each follows the same right, left, and unspecified laterality pattern as the M25.56x knee pain codes.
Each one has a clean billing trigger:
- Effusion (M25.461 right, M25.462 left, M25.469 unspecified): Bill when joint swelling is documented alongside the pain. Effusion is a common companion finding on a knee exam.
- Hemarthrosis (M25.061, M25.062, M25.069): Bleeding into the joint, typically post-injury or post-procedure. The documentation has to support actual blood in the joint, not just swelling.
- Stiffness (M25.661, M25.662, M25.669): A secondary code when range-of-motion limitation is documented as its own finding, separate from the pain.
The laterality discipline carries straight across all three. If the note names the side, the code names the side. The unspecified options exist for the same narrow reason they do in the pain family, a record that doesn't document which knee.
On the stability question coders ask every fall: the FY2027 ICD-10-CM release published in June 2026 adds 190 new diagnosis codes effective October 1, 2026. Confirm the M25.56x knee pain family against the FY2027 addendum during the annual refresh, since that's the authoritative source for any carry-forward check.
The Coordination and Maintenance Committee materials behind each release sit on the CMS C&M materials page.
Knee Pain Coding and Your Revenue Cycle
Knee pain coding errors are a revenue problem, not just a compliance one. Unspecified-code overuse, missing laterality, and undercoding after a confirmed diagnosis each generate preventable denials. For orthopedic and therapy practices, clean knee pain coding directly affects how fast claims get paid.
The leak is rarely one big error. It's the same small mistakes repeating across a high volume of musculoskeletal claims, each one a denial or a delay that staff has to chase. Twenty unspecified-code denials a month is the kind of pattern that drags down a practice's cash flow without ever showing up as a single alarming number.
Three habits close most of the gap:
- Certified coding review on musculoskeletal claims before submission.
- Laterality verification on every claim, so the side on the chart is the side on the code.
- Code-upgrade discipline as the diagnosis evolves, moving from M25.56x to M17 or S83 the day a cause is confirmed.
Where MedSole RCM fits
Orthopedic, physical therapy, occupational therapy, and pain management practices billing M25.561, M25.562, M17.x, and S83.x codes can outsource the full cycle. MedSole RCM bills at 2.99% of collections, against the 7 to 10% typical of specialty orthopedic billing firms, with no setup fees, no long-term contracts, and a 99% clean claim rate. Provider credentialing runs $99 per payer across 900-plus payer networks in all 50 states, with more than 4,000 providers credentialed. The team tracks every ICD-10-CM release, including mid-year updates like April 1, 2026, so claims never run against a stale rule set. The billing side is detailed on the outsourced medical billing services page, and credentialing is covered under provider enrollment and credentialing services.
Knee Pain ICD-10 Coding: Frequently Asked Questions
What is the ICD-10 code for knee pain?
The ICD-10-CM codes for knee pain are M25.561 for the right knee, M25.562 for the left knee, and M25.569 when the side isn't documented. M25.56 is the non-billable parent, so every claim carries one of the three child codes. The same ICD-10 cluster logic shows up in MedSole's abdominal pain ICD-10 guide.
Is M25.56 a billable code?
No. M25.56 lacks the required sixth character for laterality, so it isn't billable. A claim needs M25.561, M25.562, or M25.569. Submitting the parent code triggers an automatic specificity edit from every payer.
How do you code bilateral knee pain?
Report both M25.561 and M25.562 on the same claim. No single bilateral knee pain code exists, and Official Guidelines Section I.B.13 directs coders to assign separate codes for the left and right side when no bilateral code is provided. M25.569 is never the bilateral answer.
What is the ICD-10 code for chronic knee pain?
There's no dedicated code. Pair the laterality code, M25.561 or M25.562, with G89.29 (other chronic pain) when the provider documents chronicity. Sequencing follows visit purpose: the knee code first for treatment visits, G89.29 first for pain-management encounters.
Does anyone still use ICD-9 for knee pain?
No. ICD-9 retired for HIPAA-covered claims on October 1, 2015. The legacy code 719.46 (pain in joint, lower leg) was replaced by M25.561, M25.562, and M25.569. ICD-9 codes appearing in a billing system today are mapping errors that auto-reject.
What's the difference between a knee pain code and an osteoarthritis code?
A knee pain code is a symptom code, used before a diagnosis is established. Once the provider confirms osteoarthritis, the M17 code with laterality replaces it as primary, per the symptom-coding rules in Sections I.B.4 and I.B.5. Carrying both after confirmation is a redundancy error.
Key Takeaways for 2026 Knee Pain Coding
Knee pain coding comes down to specificity: M25.561 for the right knee, M25.562 for the left, both codes for bilateral, and M25.569 only when the side isn't documented. Five rules carry the rest.
- Use the laterality code over M25.569 whenever the side is charted. Payer edits now deny the lazy default.
- Bilateral is always two codes, M25.561 plus M25.562, per Section I.B.13. No combined code exists.
- Upgrade to M17 or S83 the day a diagnosis is confirmed. The symptom code retires.
- Chronic pain pairs G89.29 with the laterality code, sequenced by visit purpose.
- The April 1, 2026 release is the active rule set through September 30, 2026, with the knee pain family unchanged.
Get those five right and most knee pain denials never reach your desk. The codes are simple once the documentation and the laterality discipline behind them hold up.