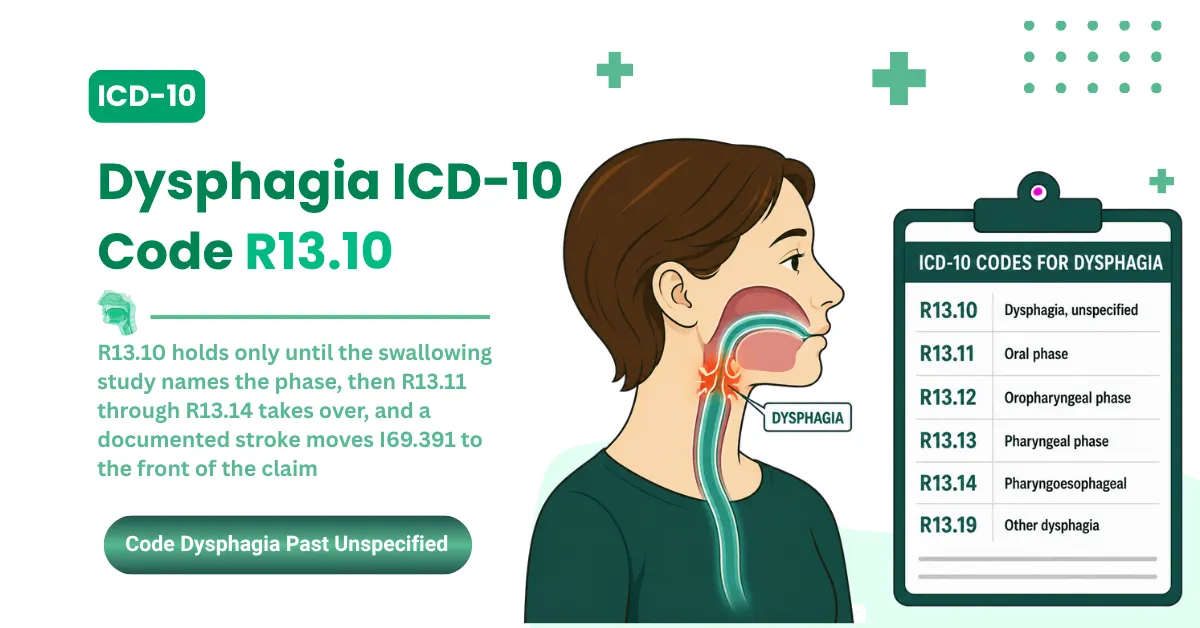


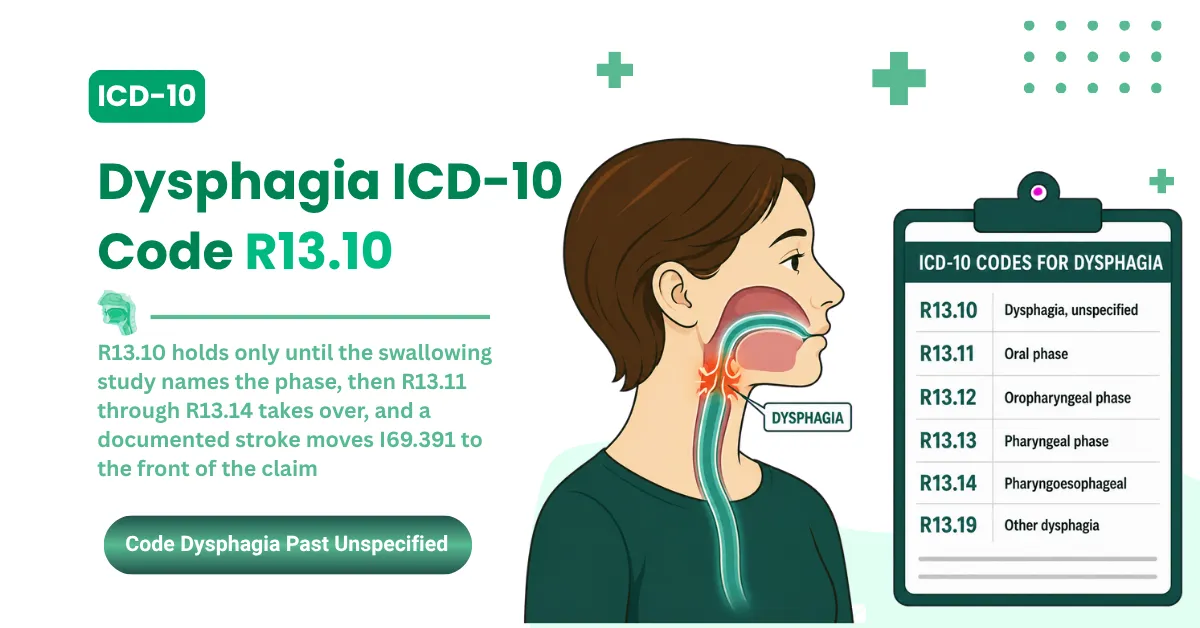
The ICD-10 code for dysphagia is R13.10 when the swallowing phase isn't documented. It's the unspecified code, and it's billable. The catch is the parent code above it. R13.1 on its own won't pay.
Here's what trips up most claims. Dysphagia coding isn't one code. It's a family, and the right one depends on two things: whether the swallowing phase is documented, and whether a cause like a stroke is on the chart.
Pick wrong and the claim either denies or invites an audit. Pick right and it pays the first time.
This guide walks the full R13 family, the post-stroke I69 codes, the aspiration pairing with J69.0, the CPT crosswalk, and the denial patterns that cost practices the most.
What Is the ICD-10 Code for Dysphagia?
The ICD-10 code for dysphagia is R13.10 for the unspecified type, with five more specific codes (R13.11 through R13.19) for when the swallowing phase is documented. R13.10 is billable. The parent code, R13.1, is not, so every claim needs a four-character code.
That parent-code rule catches more practices than anything else. Drop R13.1 on a claim by itself and it rejects at the clearinghouse before a payer ever sees it. The fix is simple once you know it: always go to the fourth character.
Dysphagia falls under Chapter 18 of ICD-10-CM, the symptoms and signs chapter (codes R00 through R99). That placement matters for billing, and we'll come back to why when we cover the stroke and esophageal codes.
The phase-specific codes
When the chart documents which phase of the swallow is affected, you move off R13.10 to a specific code:
- R13.11: Oral phase. The problem is forming or moving the food before the swallow starts.
- R13.12: Oropharyngeal phase. This is the one billed most often, common after stroke.
- R13.13: Pharyngeal phase. Often tied to aspiration risk.
- R13.14: Pharyngoesophageal phase. Upper esophageal sphincter problems land here.
- R13.19: Other dysphagia. Cervical and neurogenic dysphagia route here per the Alphabetic Index.
Specify When You Can: Defaulting to R13.10 on every visit when the note names the phase invites medical necessity review. If the swallowing study identifies the phase, the claim should reflect it.
One more rule before the codes get more complex. Swallowing is a complicated process, somewhere around 50 pairs of muscles working in sequence, per the NIDCD Dysphagia fact sheet. That's why the phase matters, and why payers expect specificity once it's on the chart. The CDC ICD-10-CM browser confirms R13.10 as the unspecified entry, and AAPC's reference places it under the R13 range.
FY2026 Updates Every Provider Billing Dysphagia Should Know
Most billing teams refresh their code files once a year, every October 1. That habit is the problem. ICD-10-CM had a mid-year update on April 1, 2026, and a lot of practices missed it.
Here's what that means for a dysphagia claim. The April 1, 2026 release is the active code set for every date of service from April 1 through September 30, 2026. The companion Official Guidelines carry an "Updated April 1, 2026" stamp.
Now the part that matters for R13: nothing in the dysphagia family changed. The April update touched instructional notes, not codes. No new dysphagia codes, no deletions, no revisions. R13.10 through R13.19 are exactly what they were, and the I69 post-stroke codes held steady too.
So why bring it up? Because running June claims on the October file can still trigger invalid-code rejections on the system side, even when your code selection is perfect. The diagnosis is right. The file is stale. The claim bounces anyway.
Check Your File Date: Confirm your practice management system loaded the April 1, 2026 release before you submit any claim dated after April 1. A correct code on an outdated file still rejects.
Looking further out, the FY2027 files are already published, effective October 1, 2026. The R13 dysphagia family carries forward unchanged in what's been released so far. Your current workflow holds, but the file date is worth a check each cycle.
CMS posts the update on its ICD-10 codes page, and the guidelines live on the CDC's ICD-10-CM files page. Both confirm the R13 codes below.
|
ICD-10 Code |
Description |
Effective Date |
|---|---|---|
|
R13.10 |
Dysphagia, unspecified |
October 1, 2025 |
|
R13.11 |
Dysphagia, oral phase |
October 1, 2025 |
|
R13.12 |
Dysphagia, oropharyngeal phase |
October 1, 2025 |
|
R13.13 |
Dysphagia, pharyngeal phase |
October 1, 2025 |
|
R13.14 |
Dysphagia, pharyngoesophageal phase |
October 1, 2025 |
|
R13.19 |
Other dysphagia |
October 1, 2025 |
|
I69.391 |
Dysphagia following cerebral infarction |
October 1, 2025 |
|
J69.0 |
Aspiration pneumonia |
October 1, 2025 |
Complete Dysphagia ICD-10 Code Reference: R13.10 Through R13.19
Every dysphagia claim comes down to picking one code from this family. Get the phase right and the claim supports the therapy and the studies behind it. Get it vague and you've capped what the claim can justify.
R13.0 vs R13.10: the distinction that prevents a denial
Before you reach for R13.10, check one thing: can the patient swallow at all?
R13.0 is aphagia, the complete inability to swallow. R13.10 is dysphagia unspecified, difficulty swallowing when some swallowing still happens. They aren't interchangeable, and the chart has to match the code.
Bill R13.10 when the note says "unable to swallow" and you've got a mismatch that surfaces in an audit. Bill R13.0 when the note only says "difficulty," and you've claimed more severity than the record supports.
Read the Words on the Chart: If the provider wrote "unable to swallow," use R13.0. If the note says "difficulty swallowing" or "dysphagia," use the right R13.1x code. The two never belong on the same claim.
The six billable subcodes and when each applies
Each subcode maps to a phase of the swallow. The more specific the code, the stronger the medical necessity behind the services on the claim.
|
Code |
Description |
Use When |
Billing Consequence |
|---|---|---|---|
|
R13.10 |
Dysphagia, unspecified |
Diagnosed, no phase identified yet; initial visit before a swallow study |
Fine short-term; long-term use without a phase update draws scrutiny and prior-auth pushback |
|
R13.11 |
Dysphagia, oral phase |
Note shows trouble forming or moving the bolus, anterior spillage, weak tongue control |
Supports CPT 92610, the clinical swallow exam; documents oral motor impairment for therapy |
|
R13.12 |
Dysphagia, oropharyngeal phase |
Combined oral and pharyngeal dysfunction; residue in the valleculae or pyriform sinuses on imaging |
Most billed phase code; supports MBSS and FEES (CPT 92611, 92612); common post-stroke |
|
R13.13 |
Dysphagia, pharyngeal phase |
Delayed swallow reflex, weak pharyngeal contraction, aspiration after the swallow |
Supports aspiration risk documentation; pairs with J69.0 when aspiration is confirmed |
|
R13.14 |
Dysphagia, pharyngoesophageal phase |
UES dysfunction, cricopharyngeal bar on imaging, globus with a confirmed UES problem |
Supports necessity for esophageal dilation (CPT 43450, 43453) and Botox injection |
|
R13.19 |
Other dysphagia |
Cervical dysphagia, neurogenic dysphagia, or a type that doesn't fit R13.11 through R13.14 |
Per the Alphabetic Index, cervical and neurogenic dysphagia route here |
R13.1 as a bare three-character code isn't billable. Submit it without the fourth character and it draws an automatic edit rejection from every payer, no matter how good the documentation is. Always go to R13.10, R13.11, R13.12, R13.13, R13.14, or R13.19.
Quick reference for the subcodes:
- R13.10: unspecified, the common starting code
- R13.11: oral phase, bolus control
- R13.12: oropharyngeal phase, billed most often
- R13.13: pharyngeal phase, aspiration focus
- R13.14: pharyngoesophageal phase, the UES code
- R13.19: other, cervical and neurogenic
ASHA's ICD-10 reference confirms the R13.1 series for dysphagia and flags when the I69 sequelae codes take over for post-stroke cases, which is where we're headed next.
Dysphagia ICD-10 Codes Beyond R13: Post-Stroke, Esophageal, and Aspiration
R13 covers dysphagia as a symptom. Once a cause is on the chart, the coding often moves to a different chapter entirely. Three situations pull dysphagia out of R13: a stroke, an esophageal problem, and aspiration. Each one has its own rule.
Post-stroke dysphagia and the I69 codes
When dysphagia follows a stroke, R13 isn't the lead code anymore. Category I69, sequelae of cerebrovascular disease, takes over.
The rule comes straight from the Official Guidelines. I69 reports the deficits that stick around after the stroke itself has resolved, and dysphagia is one of them. The I69 code sequences first. An R13.1x phase code can follow as secondary, but only when the swallow study documents the phase.
Reverse that order and you've got the most common post-stroke dysphagia denial there is. R13 in the primary slot when a stroke is the documented cause reads as a sequencing error to the payer.
|
Stroke Type Documented |
I69 Code |
When to Use |
|---|---|---|
|
Cerebral infarction (ischemic) |
I69.391 |
Dysphagia as a sequela of ischemic stroke |
|
Subarachnoid hemorrhage |
I69.091 |
Dysphagia after nontraumatic subarachnoid hemorrhage |
|
Intracerebral hemorrhage |
I69.191 |
Dysphagia after nontraumatic intracerebral hemorrhage |
|
Other nontraumatic intracranial hemorrhage |
I69.291 |
Dysphagia after other nontraumatic intracranial hemorrhage |
|
Other specified cerebrovascular disease |
I69.891 |
Dysphagia after other specified CVD |
|
Unspecified cerebrovascular disease |
I69.991 |
Dysphagia after unspecified CVD |
Sequence I69 First: On any post-stroke dysphagia claim, the I69 code leads. Add R13.12 or another phase code second when the study documents the phase. Lead with R13 and the claim trips a sequencing edit.
Esophageal dysphagia and the K22 codes
Esophageal dysphagia sits in a different chapter than the oropharyngeal type. Per AAPC's classification, esophageal dysfunction codes live in Chapter 11, the digestive system, not Chapter 18.
K22.2 is esophageal obstruction, the code for a structural block: a Schatzki ring, a web, a stricture, or a tumor. K22.4 is dyskinesia of the esophagus, the motility code for achalasia, diffuse spasm, or nutcracker esophagus.
GERD is the most common digestive cause of trouble swallowing, and it codes alongside the esophageal code, not instead of it. The reflux side runs on K21.9, K21.00, or K21.01, while K22.2 or K22.4 captures the structural or motility piece. MedSole's guide to the GERD ICD-10 code K21.9 covers the reflux billing in full.
One more pairing worth a flag. Patients with pill-induced esophageal injury sometimes show elevated liver enzymes on the same workup, billed separately under the ICD-10 code for transaminitis R74.01 when the provider documents and addresses it.
Aspiration pneumonia and the J69.0 pairing
J69.0 is aspiration pneumonia, and it's the companion code that carries the most clinical weight in dysphagia billing. When the chart documents aspiration, including silent aspiration caught on a swallow study, J69.0 rides alongside the dysphagia code.
The two-code order is simple. Code the dysphagia first, either R13.13 for the pharyngeal phase or I69.391 for a post-stroke cause, then add J69.0 second. No single code combines them, so the pair is the answer for dysphagia with aspiration.
Document the Aspiration: J69.0 needs aspiration in the record, either seen at the bedside or confirmed on a study. Risk alone won't support it. Silent aspiration counts when the study report names it.
The post-stroke sequencing framework comes from the ICD-10-CM Official Guidelines, and the NIDCD fact sheet confirms aspiration pneumonia as a leading complication of untreated dysphagia.
How to Pick the Right Dysphagia ICD-10 Code: A Three-Question Framework
Choosing the dysphagia code comes down to three questions in order. Skip one and that's usually where the error creeps in. Here's the sequence.
Question 1: Is dysphagia confirmed?
The Guidelines let you code a symptom when no definitive diagnosis is established yet. For dysphagia, that splits two ways.
If the provider wrote "dysphagia" or "difficulty swallowing," R13.x is in play. Move to question 2. If the note says "possible dysphagia" or "rule out dysphagia" in an outpatient setting, you don't code it as confirmed. Outpatient rules don't allow coding a suspected diagnosis as if it's certain.
Inpatient is the exception. There, a probable or suspected diagnosis can be coded as confirmed, which is a real difference between the two settings.
Don't Overreach on Certainty: Code to what the note supports, nothing more. R13.10 is the honest choice when the phase isn't documented. It's not a shortcut, it's the correct call when specificity isn't there.
Question 2: Is the swallowing phase documented?
Once dysphagia is confirmed, the phase decides the code:
- No phase documented goes to R13.10
- Oral phase goes to R13.11
- Oropharyngeal phase goes to R13.12
- Pharyngeal phase goes to R13.13
- Pharyngoesophageal phase goes to R13.14
- A documented phase that doesn't fit the above goes to R13.19
Update After the Study: When an MBSS or FEES names the phase after you started with R13.10, move to the specific code for the next claims. Note the date of the change in the record. Billing R13.10 after a study confirmed the phase is the pattern auditors look for.
Question 3: Is there a documented cause?
If a cause is on the chart, it changes the lead code:
- Post-stroke goes to I69.391 first, R13.1x second
- GERD causing esophageal dysphagia goes to K21.9 first, K22.4 second
- Esophageal stricture goes to K22.2 first
- Parkinson's with dysphagia goes to G20 first, R13.1x second
Outpatient vs inpatient at a glance
|
Setting |
What the Note Says |
Code |
|---|---|---|
|
Outpatient |
"Dysphagia" (confirmed) |
R13.10, or phase code if documented |
|
Outpatient |
"Possible dysphagia" |
Code the symptom, the difficulty swallowing |
|
Outpatient |
"Dysphagia following CVA" |
I69.391 first, R13.1x second if phase documented |
|
Inpatient |
"Probable dysphagia" |
R13.10, coded as confirmed under inpatient rules |
|
Inpatient |
"Suspected post-stroke dysphagia" |
I69.391, coded as confirmed under inpatient rules |
This framework catches most of the coding errors before they reach a payer. When the volume gets high enough that a manual check on every claim isn't realistic, that's the point most practices bring in help. MedSole RCM runs this kind of code-to-documentation check on every claim through its outsourced medical billing services, which is where the recurring R13.10 denials tend to stop.
CPT Codes That Pair With Dysphagia ICD-10 Codes
A dysphagia code rarely travels alone on a claim. Every service billed with it has to be justified by the diagnosis, and the diagnosis has to be specific enough to carry the procedure. A vague code can't anchor an expensive study.
The diagnostic and evaluation codes
These are the CPT codes that lean on R13.x or I69.391 as the linked diagnosis:
|
CPT |
Procedure |
Dysphagia Code Pair |
Medical Necessity Threshold |
|---|---|---|---|
|
92610 |
Clinical swallow evaluation (bedside) |
R13.10, R13.11, R13.12, R13.13 |
Documented symptoms; the first eval before any instrumental study |
|
92611 |
Swallow study with videofluoroscopy (MBSS) |
R13.10, R13.12, R13.13, I69.391 |
Aspiration risk or failed conservative care; follows a clinical exam |
|
92612 |
Endoscopic swallow evaluation (FEES) |
R13.12, R13.13, R13.14, I69.391 |
Pharyngeal or aspiration concern needing direct view |
|
92616 |
FEES with laryngeal sensory testing |
R13.13, R13.14 |
Sensory testing alongside the swallow evaluation |
|
92526 |
Swallowing therapy treatment |
R13.10, R13.11, R13.12, R13.13 |
Documented dysphagia; needs a physician order for Medicare Part B |
|
99213 to 99215 |
Office visits (E/M) for dysphagia management |
R13.10, R13.12, K21.9, I69.391 |
Symptom plus diagnosis; level set by decision-making complexity |
One thing the table won't tell you: skip the investigational codes. Procedures that payers treat as investigational for dysphagia generate near-automatic denials, so they don't belong in a clean crosswalk. A focused list of what reimburses beats a long list that includes what doesn't.
Match the Procedure to the Code: Bill an MBSS with R13.10 and no documented reason for the study, and you've got a CO-50 medical necessity denial waiting. The note has to show why the instrumental study was needed at that visit, not just that dysphagia exists.
The Medicare rule behind every swallow study
Medicare coverage for swallow studies runs through CMS Billing and Coding Article A56621. It spells out the ICD-10 codes that support necessity for the swallow study CPT codes, and a few rules trip up practices that haven't read it.
A clinical exam has to come before the instrumental study. Bill an MBSS or FEES with no documented clinical evaluation first and you draw a CO-50. Place of service matters too: office, hospital, and rehab settings are covered, while mobile and home settings generally aren't for instrumental studies.
Check the Place of Service: A swallow study billed from a non-covered setting denies on the place-of-service code alone, before the diagnosis ever gets reviewed. Confirm the setting is covered before the claim goes out.
Coverage details live in CMS Billing and Coding Article A56621.
Dysphagia Claim Denials: CO-16, CO-50, and Sequencing Errors
When a dysphagia claim comes back denied, the denial code tells you where it broke. Four codes account for most dysphagia rejections across gastroenterology, neurology, and speech pathology billing. Learn to read them and you fix the cause, not just the symptom.
The four denial codes you'll see most
|
Code |
What It Means |
Why It Hits Dysphagia Claims |
The Fix |
|---|---|---|---|
|
CO-16 |
Claim lacks information |
The note doesn't confirm the dysphagia diagnosis, or the swallow study report isn't attached |
Build a pre-submission check; confirm dysphagia is stated in the assessment, not just the HPI |
|
CO-50 |
Not medically necessary |
The CPT doesn't line up with the code's specificity or the clinical indication |
Document why the study was needed: failed conservative care, aspiration risk, alarm symptoms |
|
CO-4 |
Procedure code inconsistent |
The diagnosis pointer in Box 24E doesn't support the linked CPT |
Audit the pointers before submission; I69.391 has to lead post-stroke claims |
|
Sequencing denial |
Code order violates the rules |
R13.x placed first when a stroke is the documented cause |
Put I69.391 first, R13.1x second only when the phase is documented |
Audit the Workflow, Not Just the Code: When CO-16 keeps hitting one provider's dysphagia claims, the documentation workflow is the issue, not the coding. CO-16 on dysphagia almost always means the note never states the diagnosis in the assessment, even when the phase shows up in the clinical detail.
Sequencing Is a Universal Rule: The I69-first rule isn't payer-specific. It's an Official Guidelines requirement, so it applies the same way across Medicare, Medicaid, and commercial plans. If a third of your post-stroke claims deny on sequence, the gap is team training.
Audit patterns that draw OIG attention
A few habits put dysphagia claims on an auditor's radar:
- Using R13.10 on every claim and never updating to a phase code after a study confirms one. Systematic unspecified-code use draws Targeted Probe and Educate review.
- Billing MBSS or FEES with no documented clinical exam first. Auditors look for the sequence: exam, findings, then the instrumental study.
- Copy-pasted dysphagia notes across visits. When every session shows identical language, the documentation reads as boilerplate, not patient-specific.
- Billing I69.391 with no stroke history in the chart. Coding the diagnosis up from R13.x to I69.391 without confirmed cerebrovascular disease is a known audit target.
The OIG Work Plan tracks unspecified-code overuse and post-stroke sequencing errors as recurring sources of improper payments, which is why the patterns above matter beyond a single denial.
A recurring CO-16 or CO-50 backlog on dysphagia claims usually points to documentation review that's happening after submission instead of before. The CO-16 denial code guide breaks down the information-missing pattern in detail.
How Common Is Dysphagia? The Clinical Burden Behind the Codes
Knowing how common dysphagia is does more than fill in background. It's the medical-necessity argument behind a swallow study or a course of therapy, and it's the data you reach for when a CO-50 denial needs an appeal.
Dysphagia shows up far more than most billing teams expect, especially in two populations: stroke patients and older adults. After a stroke, swallowing problems are common rather than rare, which is why I69.391 isn't an edge-case code for any neurology or rehab practice. It's a daily decision.
The same holds in elderly and long-term care populations, where dysphagia drives real downstream cost. Aspiration pneumonia is the complication that turns a swallowing problem into a hospital admission, and the NIDCD fact sheet names it as a leading complication of untreated dysphagia.
Here's why that matters for billing. When you're appealing a denied swallow study, the clinical burden is your argument. A documented aspiration risk in an older patient isn't a borderline call for an instrumental study. The risk profile supports the necessity, and the appeal should say so in those terms.
For coding teams, the takeaway is practical. High-volume dysphagia populations mean high-volume coding decisions, and small error rates compound fast. A practice seeing dysphagia daily can't afford a sloppy default to R13.10, because the same mistake repeated across hundreds of claims becomes a measurable revenue gap.
Swallowing disorders tie back to neurologic disease, GERD, stroke, and head or neck cancers, per MedlinePlus from the National Library of Medicine. That range is exactly why the coding splits across so many chapters, and why getting the lead code right takes the three-question discipline from earlier.
Dysphagia ICD-10 Coding: Frequently Asked Questions
What is the ICD-10 code for dysphagia unspecified?
R13.10 is the code for dysphagia unspecified. It means swallowing difficulty is confirmed but the specific phase hasn't been identified yet. It's billable and valid for claims. The parent code R13.1 isn't billable and can't be submitted on its own.
What is the ICD-10 code for other dysphagia?
R13.19 is the code for other dysphagia. You use it when the swallowing difficulty is specified but doesn't match the oral, oropharyngeal, pharyngeal, or pharyngoesophageal phases. Per the Alphabetic Index, both cervical dysphagia and neurogenic dysphagia route to R13.19.
What is the ICD-10 code for oropharyngeal dysphagia?
R13.12 is the code for oropharyngeal phase dysphagia, and it's the phase code billed most often. It applies when the documentation shows combined oral and pharyngeal dysfunction, including residue in the valleculae or pyriform sinuses on imaging. It shows up most in post-stroke and neuromuscular cases.
What is the ICD-10 code for dysphagia following a stroke?
I69.391 is the code for dysphagia following cerebral infarction. When a stroke is the documented cause, I69.391 sequences first, not any R13.x code. A phase code like R13.12 can follow as secondary when the swallow study documents the phase.
What is the ICD-10 code for pharyngeal dysphagia?
R13.13 is the code for pharyngeal phase dysphagia. It applies when the note shows a delayed swallow reflex, weak pharyngeal contraction, or aspiration after the swallow without much oral involvement. It's the dysphagia code most tied to aspiration risk, and it pairs with J69.0 when aspiration is confirmed.
What is the ICD-10 code for esophageal dysphagia?
Esophageal dysphagia doesn't use an R13 code. Per AAPC's classification, it uses K22.2 for a structural obstruction or K22.4 for a motility disorder like achalasia or spasm. Those codes sit in Chapter 11, the digestive system, not Chapter 18 with the symptom codes.
What is the ICD-10 code for cervical dysphagia?
Cervical dysphagia codes to R13.19, other dysphagia. It's the type tied to cervical spine problems like osteophytes, disc disease, or anterior cervical surgery. The Alphabetic Index routes it to R13.19, so document the cervical cause in the note to back up the code.
What is the ICD-10 code for dysphagia with aspiration?
There's no single code for it. You report two: the dysphagia code first, either R13.13 or I69.391 depending on the cause, then J69.0 for the aspiration pneumonia. J69.0 needs aspiration documented, and silent aspiration caught on an MBSS or FEES counts when the study names it.
Why Dysphagia Billing Starts Before You Pick the Code
Clean dysphagia coding is the output of a process, not the start of one. The claim pays when four things line up: the documentation confirms the diagnosis and phase, the code matches the record, the CPT is anchored to the right diagnosis, and the rendering provider is credentialed with the payer. Miss any one and the claim stalls.
That last piece catches people off guard. A credentialing gap throws a CO-50 that looks like a medical necessity denial but is an enrollment problem at its root. The coding was fine. The provider just wasn't loaded with the payer yet.
The Pre-Submission Rule: A dysphagia claim that hasn't passed a documentation check, a code-accuracy review, a CPT-alignment look, and a credentialing confirmation before it goes out is a claim that pays on luck. Build the checks in and luck stops being part of it.
Where MedSole RCM fits
Gastroenterology, neurology, internal medicine, and speech pathology practices billing dysphagia every day can hand off the whole cycle. MedSole RCM bills at 2.99% of collections, against the 7 to 10% that specialty outpatient firms typically charge, with no setup fees and no long-term contracts. The clean claim rate runs at 99%. Provider credentialing runs $99 per payer across 900-plus payer networks in all 50 states, with more than 4,000 providers credentialed. The team tracks every ICD-10-CM release, including mid-year updates like April 1, 2026, so dysphagia claims never run against a stale code file. The full picture is on the outsourced medical billing services page, and the credentialing side is covered under provider enrollment and credentialing services.
The dysphagia code decision in five lines
- Use R13.10 when dysphagia is confirmed but the phase isn't documented.
- Use R13.11 through R13.14 when the swallow study names the phase.
- Use R13.19 when the type is specified but doesn't fit the listed phases.
- Use I69.391 first when a stroke is the documented cause, R13.x second.
- Use K22.2 or K22.4 when the cause is esophageal, not a symptom code.
Get those five right and most dysphagia denials never happen. The code is the easy part once the documentation and the workflow behind it are solid.