_11zon.webp)


_11zon.webp)
The ICD-10 code for cough is R05.9 (cough, unspecified) when no duration is documented, R05.1 (acute cough, less than 3 weeks), R05.2 (subacute cough, 3 to 8 weeks), R05.3 (chronic cough, more than 8 weeks), R05.4 (cough syncope), or R05.8 (other specified cough). R05 without a decimal isn't billable.
That last line is where claims break. Drop a bare R05 on a claim and it trips a specificity rejection at the clearinghouse before a payer sees it.
Here's the currency piece. The active code set is the FY2026 release, with the April 1, 2026 update covering services through September 30, 2026. That update changed instructional notes only, zero new diagnosis codes, and the R05 family is untouched.
This guide walks every billable R05 code, the Excludes rules that block claims, the CPT pairings, and the documentation habits that keep cough claims clean.
What Is the ICD-10 Code for Cough? The R05 Family and Why R05 Alone Fails
In ICD-10-CM, R05 is the parent category for cough, but it isn't a billable code. Since the October 1, 2021 expansion, every cough claim needs a specific subcode: R05.1 for acute, R05.2 for subacute, R05.3 for chronic, R05.4 for cough syncope, R05.8 for other specified, or R05.9 for unspecified.
The 2022 restructuring that changed cough coding
Before October 1, 2021, every cough used a single billable code: plain R05. That changed with FY2022.
The American Thoracic Society and the American College of Chest Physicians pushed the expansion through the ICD-10 Coordination and Maintenance Committee, arguing that duration drives the differential. Effective October 1, 2021, R05 became a non-billable parent with six children below it.
So here's the correction worth flagging. Any article still saying "the cough code is R05" is quoting retired guidance. That single code has been dead for claims since 2021, and a system that submits it gets the claim kicked back. The same FY2022 cycle split other families the same way, including low back pain, where M54.5 broke into M54.50, M54.51, and M54.59. MedSole's back pain ICD-10 guide covers that parallel split, and the broader shift is in the ICD-10 vs ICD-11 guide.
The six billable codes that replaced the single code
The full family looks like this, with the duration thresholds most quick references leave out:
- R05.1: Acute cough, less than 3 weeks
- R05.2: Subacute cough, 3 to 8 weeks
- R05.3: Chronic cough, more than 8 weeks
- R05.4: Cough syncope, with a code-first note for R55
- R05.8: Other specified cough, including drug-induced and psychogenic
- R05.9: Cough, unspecified, only when no duration is documented
The Official Guidelines push you to the highest specificity the documentation supports. When the chart names a duration, the unspecified code stops being defensible, which is exactly where the next section starts.
The change ran through the CDC's September 2020 Coordination and Maintenance meeting, posted on the CMS ICD-10 page and the CDC's ICD-10-CM files page, with the full R05 family detailed at icd10data.
R05.9: Cough Unspecified, When It's Valid and When It's an Audit Risk
R05.9 (cough, unspecified) is a valid, billable code for 2026, but treat it as a last resort. It fits only when the note doesn't document duration, type, or associated features, which makes a more specific code impossible to assign.
There's a defensible use for it. On an initial visit, when the cough is new and nobody's pinned down how long it's been going, R05.9 is the honest code. The Guidelines recognize that unspecified codes have legitimate uses when the detail isn't there yet.
The problem starts when duration shows up in the note and R05.9 stays on the claim anyway. "Cough for two weeks" anywhere in the chart forces R05.1. The code has to match the highest specificity the documentation supports, and a two-week note supports acute, not unspecified.
Repeated R05.9 on charts that contain duration language is where it turns into a pattern. That mismatch between documentation and coding is what payers' automated edits flag. Symptom-code specificity also sits in the OIG's compliance focus, so a habit of defaulting to unspecified is the kind of thing that surfaces in an audit.
Duration Kills R05.9: The moment any duration appears in the note, the HPI included, R05.9 stops being defensible. "Cough for five days" is an R05.1 claim, even if the assessment line says only "cough."
The same unspecified-code logic runs across all of Chapter 18. MedSole's abdominal pain ICD-10 guide walks the identical audit pattern on the R10.9 side, where the unspecified code draws the same scrutiny. The full R05.9 detail sits at AAPC, and the unspecified-code guidance is in the ICD-10-CM Official Guidelines.
R05.1: Acute Cough, the J06.9 Distinction, and the COVID Crosswalk
R05.1 is the code for acute cough, one the provider documents as lasting less than three weeks. It applies to an isolated cough with no confirmed upper respiratory infection, when duration is on the chart but no underlying cause has been established.
The three-week rule does the work here. Any stated timeframe supports R05.1, even something as loose as "cough since Tuesday." No timeframe at all sends you back to R05.9. The duration is the deciding fact, not the wording around it.
Now the distinction that trips up urgent care billing: R05.1 versus J06.9. An isolated cough with no pharyngitis, no rhinorrhea, and no sinus symptoms is R05.1, never J06.9. J06.9 claims a multi-symptom upper respiratory infection, and billing it for a lone cough asserts a diagnosis the note doesn't support. That mismatch is a top edit flag.
Sole-Complaint Rule: When cough is the only documented complaint, R05.1 is the code. J06.9 needs multiple documented upper respiratory symptoms, so billing it for an isolated cough creates a clinical mismatch the payer can see.
There's a COVID angle too. When COVID-19 is suspected but not confirmed, the FY2026 Official Guidelines point to the symptom code for the cough rather than a confirmed-diagnosis code. The current guidance lives in the April 1, 2026 edition, so code from that version rather than an older copy.
One common question fits here. A "hacking cough" has no dedicated code. Duration picks the code, not the character of the cough, so a hacking cough under three weeks is still R05.1.
R05.3: Chronic Cough, the Most Scrutinized Code in the R05 Family
R05.3 is the code for chronic cough, one the provider documents as lasting more than eight weeks. It draws more payer scrutiny than any other R05 code, because repeated R05.3 billing with no documented workup of the treatable causes invites medical-necessity review.
Duration, plus the inclusion-term most billers miss
Exact duration in weeks or months supports R05.3 without trouble. That's the bulletproof habit.
Here's the part most references get wrong. The R05.3 code also covers "persistent," "refractory," and "unexplained" cough as inclusion terms. So a note documenting "persistent cough" indexes straight to R05.3, not to R05.9 as a fallback. If the chart says persistent and you code unspecified, you've undercut your own claim. When the duration is spelled out, even better, but the inclusion terms carry it on their own.
The three-cause workup payers look for
Chronic cough has three common treatable causes, and this is where the scrutiny comes from. The ACCP and CHEST clinical guidelines name upper airway cough syndrome, asthma, and GERD as the big three. Payers reviewing repeated R05.3 claims look for documented evaluation or active management of those causes.
One clarification matters here, because plenty of sources get it wrong. This is guideline-driven, not a named Medicare mandate. No CMS rule says "work up these three before billing R05.3." The pressure is medical-necessity review on repeated claims, and the defense is documentation showing the causes were considered.
When the etiology code replaces R05.3
Once a cause is confirmed, the etiology code takes the primary slot and R05.3 steps down. GERD codes as K21.9, K21.00, or K21.01, since K21.0 on its own isn't billable. Asthma codes as J45.x. Upper airway cough syndrome codes as J31.0. Per the Chapter 18 symptom rule, the symptom code drops once the definitive diagnosis is established.
Etiology Replaces Symptom: The day the EGD, spirometry, or ENT workup confirms a cause, R05.3 stops being the primary diagnosis. Carrying it as primary after a confirmed etiology is a redundancy edit waiting to fire.
Medical-necessity denials on R05.3 diagnostics are their own headache, broken down in MedSole's CO-50 denial code guide. When reflux is the confirmed cause, the GERD ICD-10 code guide covers the K21 side, and the full R05.3 detail is at AAPC.
R05.2, R05.4, and R05.8: Subacute, Cough Syncope, and Drug-Induced Cough
Three codes in the R05 family handle the less common presentations: R05.2 for the subacute window of 3 to 8 weeks, R05.4 for cough syncope with a required code-first note for R55, and R05.8 for drug-induced or neuropathic cough. Each carries a rule worth knowing.
R05.2: the window nobody codes
R05.2 covers the middle ground, 3 to 8 weeks, and it's the most under-used of the three. A 5-week post-viral cough isn't acute anymore and isn't chronic yet. It's subacute, and it's R05.2. The code sits in DRG 204, respiratory signs and symptoms, under MS-DRG v43.0.
R05.4: the code that's never first
R05.4 is cough syncope, and it comes with two rules that point the same way. First, it carries a code-first note for R55, syncope and collapse, so R55 leads whenever both are documented. Second, the Medicare Code Editor flags R05.4 as an unacceptable principal diagnosis, so it can't be the first-listed code on a claim, full stop. The note also has to state the syncope was triggered by the coughing, not just present at the same time.
R05.4 Is Never First: Between the code-first R55 note and the Medicare Code Editor's unacceptable-principal-diagnosis edit, R05.4 always rides second. A claim with R05.4 in the first position rejects before a human reads it.
R05.8: the drug-induced cough trap
R05.8 is other specified cough, and the classic case is the ACE inhibitor cough. That one needs two codes in order: the manifestation first, R05.8, then the adverse-effect code T46.4X5A for ACE inhibitors, initial encounter. Think lisinopril or enalapril. Billing R05.3 alone for a medication-induced cough is the single most common error on this presentation. Neuropathic cough lands here too.
The denial side of these less-common codes is where a lot of revenue leaks, which is the focus of MedSole's denial management services. For the primary-care coding angle, the hypokalemia ICD-10 guide walks a similar specificity decision, and the DRG grouping detail sits on the CMS MS-DRG v43.0 page.
Excludes1 and Excludes2 Rules for Cough Codes, and the 2021 Flip Most Sources Missed
The R05 cough family carries both Excludes1 and Excludes2 notes in the FY2026 tabular. Excludes1 means two codes can never appear on the same claim. Excludes2 means they can appear together when each condition is documented on its own. One of those notes flipped in 2021, and most sources still teach it backwards.
Excludes1: the codes you can never pair
Two conditions sit under Excludes1 for R05: paroxysmal cough due to Bordetella pertussis (A37.0-) and smoker's cough (J41.0). Confirm whooping cough or smoker's cough and that code goes on the claim alone, with R05.x off it. Pair them and you've got a hard error at the clearinghouse. The same FY2022 cycle also expanded A37 itself, splitting it into A37.00 without pneumonia and A37.01 with pneumonia.
Excludes2: hemoptysis can co-bill
Cough with hemorrhage, R04.2, sits under Excludes2. That means R05.x and R04.2 can appear together when the cough and the hemoptysis are separately documented and worked up. But when coughing up blood is the chief complaint, R04.2 is the code, not an R05.x variant.
The 2021 flip that breaks old guidance
Here's the correction that matters. Before October 1, 2021, R04.2 sat under Excludes1, the opposite rule. The FY2022 update moved it to Excludes2 at the same moment it created the six child codes. So any source built on pre-2022 guidance teaches hemoptysis co-billing backwards, telling coders to keep R04.2 and R05.x apart when the current rule allows them together. Check the date on whatever reference you're using.
|
Coding Situation |
Rule |
Action |
|---|---|---|
|
R05.x with A37.0- (pertussis paroxysmal cough) |
Excludes1 |
Never together; A37.0- only |
|
R05.x with J41.0 (smoker's cough) |
Excludes1 |
Never together; J41.0 only |
|
R05.x with R04.2 (hemoptysis) |
Excludes2, flipped from Excludes1 in FY2022 |
Together only when both are separately documented; R04.2 alone when blood is the complaint |
|
R05.x with J45.x (confirmed asthma) |
Chapter 18 symptom rule |
Drop R05.x; asthma is primary |
|
R05.x with K21.x (confirmed GERD) |
Chapter 18 symptom rule |
Drop R05.x; GERD is primary |
An Excludes1 violation is a hard denial, the kind broken down in MedSole's CO-16 denial code guide. When pneumonia and a productive cough show up together, the leukocytosis ICD-10 guide covers the lab side, and the receipt for the Excludes flip is in AAPC's 2022 cough-codes article.
Cough vs Common Cold vs URI: Coding the Differential
Cough rarely shows up alone in the real world, so the differential between R05.x, J00, and J06.9 decides a lot of claims. The rule comes down to one question: is the cough the whole story, or part of a bigger picture?
R05.x vs J00, the common cold
J00 is acute nasopharyngitis, the common cold, and it needs the full multi-symptom picture. When cough is part of a cold, it's built into J00 and you don't code it separately. But an isolated cough, even one lingering after a cold cleared, goes to R05.1.
|
Clinical Presentation |
Correct Code |
Why Not the Other |
|---|---|---|
|
Cough as sole complaint, no URI symptoms |
R05.1 (acute) or R05.3 (chronic) |
J00 needs multiple URI symptoms; an isolated cough doesn't meet the threshold |
|
Cough plus nasal congestion, sore throat, sneezing |
J00 |
Cough is integral to J00, so R05.x isn't coded separately |
R05.x vs J06.9, the unspecified URI
J06.9 covers a documented multi-symptom acute upper respiratory infection that isn't specific enough for J00 or the more detailed codes. It can't stand in for an isolated cough. That single decision rule, isolated cough goes to R05.x and a multi-symptom URI goes to J06.9, is what separates a clean claim from a mismatch.
The congestion companion codes
Congestion that's documented as its own finding rides alongside the cough code, not instead of it. Nasal congestion codes as R09.81, and other respiratory chest symptoms code as R09.89. That's how a "cough and congestion" visit captures both findings without forcing one code to carry both.
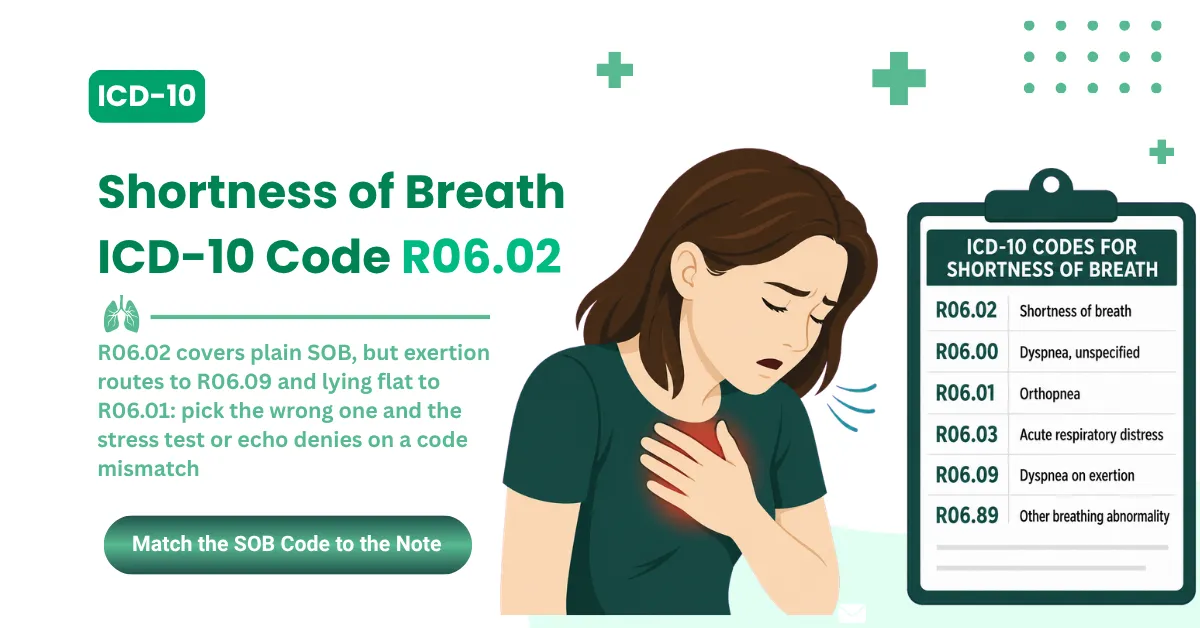
Shortness of breath often travels with these respiratory presentations, and MedSole's shortness of breath guide covers the R06.02 side of that picture.
CPT Codes That Pair With Cough ICD-10 Diagnoses: The 2026 Billing Matrix
Cough ICD-10 codes pair with CPT codes based on visit complexity and the diagnostics the presentation justifies. The diagnosis is the medical-necessity anchor for every service on the claim, and a diagnosis-to-CPT mismatch is a top denial trigger.
The working matrix breaks down like this:
|
Clinical Service |
CPT |
Cough ICD-10 Pair |
Medical Necessity Anchor |
|---|---|---|---|
|
New patient visit, straightforward MDM |
99202 / 99203 |
R05.1 |
Duration documented, no confirmed etiology |
|
Established visit, low complexity |
99213 |
R05.1 or R05.9 |
Single uncomplicated acute presentation |
|
Established visit, moderate complexity |
99214 |
R05.3 |
Multiple diagnoses reviewed, data ordered |
|
Chest X-ray, two views |
71046 |
R05.3 |
Supports the UACS, asthma, or GERD workup |
|
Spirometry |
94010 |
R05.3 |
Rules asthma in or out as the cause |
|
Rapid strep test |
87880 |
R05.1 plus J06.9 |
Rules out bacterial pharyngitis |
|
Flexible laryngoscopy |
31575 |
R05.3 |
ENT evaluation for chronic cough |
|
EGD with biopsy |
43239 |
R05.3 plus K21.9 |
GI evaluation for reflux-induced cough |
The necessity link is everything here. R05.9 trying to justify a chest CT is a CO-50 waiting to happen. R05.3 with documented failed conservative management justifies that same CT. The diagnosis and the CPT are one linked decision, not two separate boxes.
The Anchor Test: Before any diagnostic goes on a cough claim, ask what in the note makes this service necessary for this exact code. R05.9 anchors almost nothing beyond the visit itself.
MedSole RCM runs this diagnosis-to-CPT anchor check on every cough claim before it goes out, which is what the outsourced medical billing services handle day to day.
Documentation That Keeps Cough Claims Clean: The 2026 Provider Checklist
In the R05 cough family, duration is the one variable that decides the code between acute, subacute, and chronic. A provider who writes the exact duration in days or weeks kills the single most common cause of cough claim denials before the claim is even built.
Run through this checklist and the claims stay clean:
- Cough duration in days or weeks, stated outright. Decides R05.1 vs R05.2 vs R05.3.
- Whether cough is the primary complaint or secondary to a URI picture. Decides R05.x vs J00 or J06.9.
- Associated symptoms like rhinorrhea, pharyngitis, or sinus pressure, present or absent. Confirms or rules out J00 and J06.9.
- Confirmed or ruled-out underlying causes. Decides whether R05.3 stays or the etiology code takes over.
- For R05.4, an explicit statement that the coughing triggered the syncope, with R55 sequenced first.
- The current medication list, ACE inhibitors in particular. Required for the R05.8 plus T46.4X5A pairing.
- Workup status of the three causes, UACS, asthma, and GERD, on any repeat R05.3 encounter. That's the medical-necessity record.
That last item is the one that saves you in an audit. Symptom-code specificity stays an OIG compliance focus, and repeated R05.9 on charts that document duration is the pattern that surfaces. The checklist is the defense.
The full OIG compliance context lives at the OIG site.
What Unspecified Cough Codes Cost a Practice, and the Fix
Unspecified cough codes cost more than the denial rate suggests. Each R05.9 that should have been R05.1 or R05.3 isn't just one possible denial. It's a pattern that compounds across a month of high-volume cough billing into a real revenue gap.
Run the math on a busy practice. Take 200 cough encounters a month. If even one in ten carries R05.9 where the chart supported a specific code, that's 20 claims a month exposed to specificity edits, rework, and write-offs. Multiply that across a year and the leak is no longer rounding error.
The fix is three operational habits, none of them complicated:
- Build a duration prompt into the EHR cough template, so nobody can close the note without it.
- Code to the highest documented specificity on every claim, every time.
- Run a monthly R05.9-rate audit against the documentation, and coach the outliers.
Where MedSole RCM fits
Primary care, urgent care, family medicine, pulmonology, and pediatric practices billing R05.1, R05.3, R05.9, J00, and J06.9 every day can outsource the whole cycle. MedSole RCM bills at 2.99% of collections, against the 7 to 10% typical of specialty outpatient firms, with no setup fees, no long-term contracts, and a 99% clean claim rate. Provider credentialing runs $99 per payer across 900-plus payer networks in all 50 states, with more than 4,000 providers credentialed. The team tracks every ICD-10-CM release, including mid-year instructional updates like April 1, 2026, so cough claims never run against a stale rule set. The billing side is detailed on the outsourced medical billing services page, and credentialing is covered under provider enrollment and credentialing services.
Cough ICD-10 Coding: Frequently Asked Questions
What is the ICD-10 code for cough?
The ICD-10-CM codes for cough are R05.1 (acute, less than 3 weeks), R05.2 (subacute, 3 to 8 weeks), R05.3 (chronic, more than 8 weeks), R05.4 (cough syncope), R05.8 (other specified), and R05.9 (unspecified). R05 without a decimal isn't a valid billable code.
What is the 2026 ICD-10-CM diagnosis code for cough?
The 2026 cough codes run under the FY2026 release across two windows: October 1, 2025 through March 31, 2026, and the April 1, 2026 release covering services through September 30, 2026. The April update changed instructional notes only, with zero new codes, so the R05 family is identical in both windows.
Why did the cough code change in 2022?
Before October 1, 2021, every cough used a single billable code, R05. The American Thoracic Society and the American College of Chest Physicians championed a duration-based expansion through the ICD-10 Coordination and Maintenance Committee. Effective October 2021, R05 became a non-billable parent with six specific children.
What is the ICD-10 code for chronic cough?
Chronic cough codes as R05.3 when documented as lasting more than eight weeks. It's a symptom code, so once GERD, asthma, or UACS is confirmed, the etiology code replaces it as primary. Payers reviewing repeated R05.3 claims look for documented evaluation of those three causes, per ACCP clinical guidance, not a CMS mandate.
What is the ICD-10 code for a hacking cough?
A hacking cough has no dedicated code. Duration picks it: R05.1 under three weeks, R05.2 for three to eight, R05.3 beyond eight. The character of the cough, hacking, dry, or barking, gets documented for clinical accuracy but never changes the R05 selection.
Does anyone still use ICD-9 for cough?
No. ICD-9 retired for HIPAA-covered claims on October 1, 2015. The legacy cough code was 786.2, a single unspecified code, replaced by the R05 family that the October 2021 expansion then split by duration. ICD-9 codes in a billing system today are mapping errors that auto-reject.
Can I bill R05.x and J00 on the same claim?
Only when the cough is a separately documented complaint, distinct from the cold itself. When J00 is primary and the cough is part of the cold presentation, R05.x isn't coded on its own. The note has to make that distinction clear.
What are the top denial reasons for cough ICD-10 claims?
Five patterns: a bare R05 with no fourth character (automatic rejection), R05.9 used when duration is documented (specificity violation), repeated R05.3 with no documented three-cause workup, a CPT the diagnosis can't anchor (medical-necessity denial), and an Excludes1 violation pairing R05.x with A37.0- or J41.0.
Key Takeaways: 2026 Cough ICD-10 at a Glance
Cough coding lives or dies on duration: under three weeks is R05.1, three to eight is R05.2, beyond eight is R05.3. The rest comes down to five lines.
- R05 with no decimal is never billable. Always go to a subcode.
- Repeated R05.3 needs the documented UACS, asthma, and GERD workup on record. That's the medical-necessity anchor payers check.
- J00 and J06.9 aren't substitutes for an isolated cough. R05.x applies when cough is the primary complaint.
- Excludes1 bars R05.x with A37.0- or J41.0. R04.2 became Excludes2 in 2021 and can co-bill when separately documented.
- The April 1, 2026 FY2026 release is the active rule set through September 30, 2026, with instructional changes only and the R05 family untouched.
Get those five right and most cough denials never reach your desk. The coding is the easy part once the documentation behind it holds up.