

Which GERD ICD-10 Code Do You Bill? Start With One Question
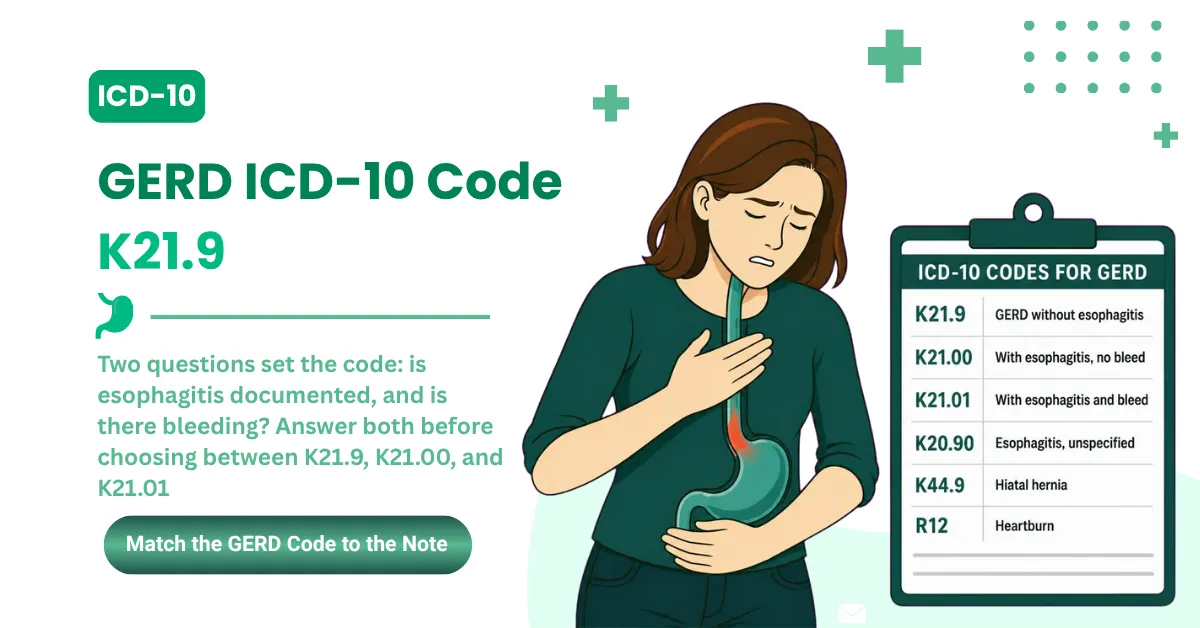
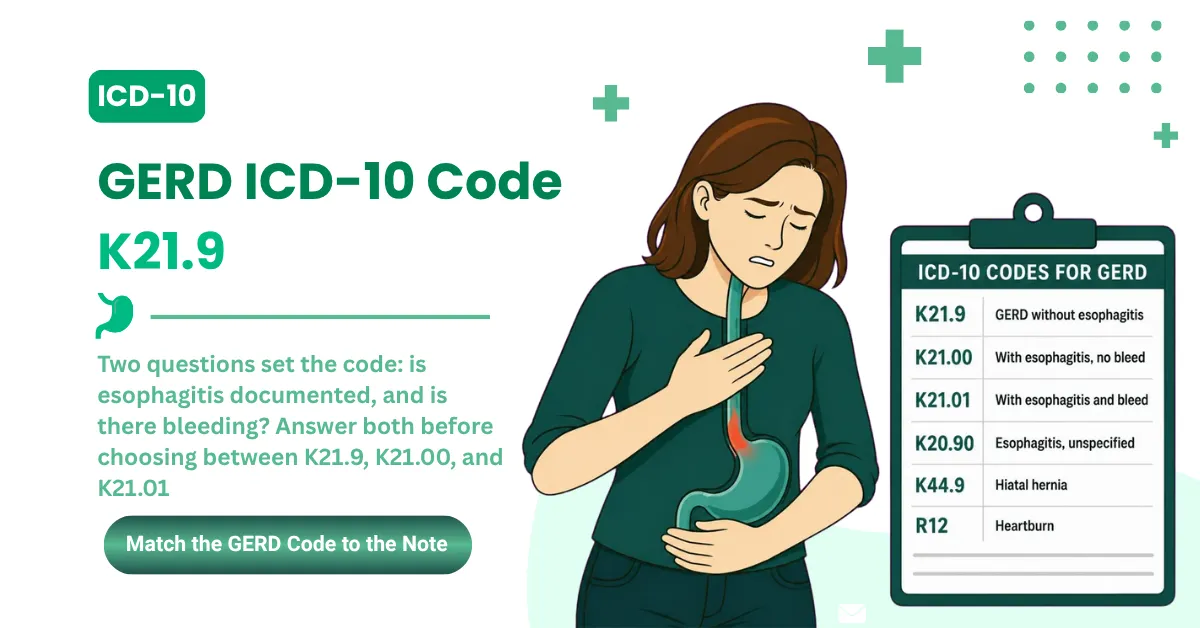
The ICD-10 code for GERD depends on one documented finding: whether esophagitis is present. Choosing the right code among K21.9, K21.00, and K21.01 determines both the reimbursement and how payers track disease severity.
Here are the three primary codes:
- K21.9 is gastroesophageal reflux disease without esophagitis. It's the most common GERD code, used when acid reflux is confirmed but no inflammation or mucosal injury appears in the medical record.
- K21.00 is GERD with esophagitis, without bleeding. Use it when an endoscopy or provider note confirms inflammation of the esophageal lining by name, with no bleeding documented.
- K21.01 is GERD with esophagitis, with bleeding. Use it when esophagitis is confirmed and bleeding, like hematemesis or GI hemorrhage, is documented by the treating provider.
A few related codes sit close to these and get mixed up with them:
- K20.90 is esophagitis, unspecified. Use it when esophagitis is documented but GERD isn't identified as the cause.
- R12 is heartburn. It applies when only the symptom is documented and no formal GERD diagnosis is made.
- K44.9 is a diaphragmatic hernia. Report it alongside K21.9 when GERD is linked to a hiatal hernia.
Specify Esophagitis Status: Always rely on the gastroenterology report or provider documentation to confirm whether esophagitis is present before choosing between K21.9 and K21.00. That one finding splits the entire code family.
Documenting Hiatal Hernias: When GERD is caused by or linked to a hiatal hernia, bill K44.9 alongside K21.9 to capture the full clinical picture and support medical necessity.
Gastroesophageal reflux disease affects about 20% of adults in the United States, according to the National Institute of Diabetes and Digestive and Kidney Diseases. That volume is why these codes show up across primary care, internal medicine, and gastroenterology billing every day.
The CDC ICD-10-CM browser tool and the CMS FY2026 Official Guidelines govern K21.9 validity for HIPAA-covered transactions through September 30, 2026.
K21.9, K21.00, K21.01 Side by Side, Plus 11 Related Codes Coders Confuse Them With
Selecting the correct GERD ICD-10 code requires answering two clinical questions in sequence: Is esophagitis documented? If yes, is bleeding documented? Those two answers route every GERD claim to the right code.
The three primary K21 codes
|
ICD-10 Code |
Official Description |
Use When |
Billing Consequence |
|---|---|---|---|
|
K21.9 |
GERD without esophagitis |
GERD diagnosed, no esophagitis documented |
Supports E/M 99213 to 99215 and outpatient medication management. Can't alone justify EGD with biopsy (43239) |
|
K21.00 |
GERD with esophagitis, without bleeding |
Esophagitis confirmed by name, no bleeding documented |
Supports EGD (43235 to 43239) and biopsy justification. Needs documented esophagitis |
|
K21.01 |
GERD with esophagitis, with bleeding |
Esophagitis confirmed and bleeding documented |
Supports endoscopic hemostasis (CPT 43255), shifts the inpatient DRG, needs documented bleeding |
Neither K21 nor K21.0 is billable. K21 has three characters, K21.0 has four, and K21.0 needs a fifth digit to become K21.00 or K21.01. Submit either parent code and it triggers an automatic specificity edit from every payer before a human reviews the claim.
Related, companion, and differential codes
These eleven codes sit next to the K21 family, and each one has a clear rule for when it applies instead of or alongside K21.9.
|
ICD-10 Code |
Description |
When to Use Alongside or Instead of K21.9 |
|---|---|---|
|
K20.90 |
Esophagitis, unspecified, without bleeding |
Esophagitis documented but the provider doesn't name GERD as the cause. Never combine with K21.00, they're mutually exclusive |
|
K21.1 |
GERD with esophageal stricture |
Long-standing GERD with documented narrowing. Supports necessity for dilation (CPT 43450, 43453) |
|
K21.8 |
Other gastro-esophageal reflux disease |
Rare. Documented GERD complications that don't fit K21.9, K21.00, or K21.01. Not a default fallback |
|
K22.70 |
Barrett's esophagus without dysplasia |
Barrett's takes its own code. Don't code K21.9 for Barrett's, use K22.70 and add K21.x for concurrent GERD |
|
K22.4 |
Esophageal stricture |
Peptic stricture from chronic untreated GERD when the stricture is the primary finding |
|
K44.9 |
Diaphragmatic hernia without obstruction |
Alongside K21.9 when a hiatal hernia contributes to GERD. May sequence first if the hernia is primary |
|
R12 |
Heartburn |
Only when heartburn is documented and GERD hasn't been diagnosed. Once K21.9 is assigned, never add R12, it's integral to GERD and creates a redundant-code edit |
|
P78.83 |
Neonatal esophageal reflux |
Neonates 0 to 28 days use P78.83. Billing K21.9 for a neonate generates a code-age conflict rejection |
|
Z87.19 |
Personal history of other digestive diseases |
Only when GERD is documented as resolved. Never report it for an active GERD encounter, and never alongside K21.x |
|
K22.10 |
Esophageal ulcer without hemorrhage |
Esophageal ulcer documented separately from esophagitis. May accompany K21.00 |
|
T47.1X5A |
Adverse effect of antacids or PPIs, initial encounter |
Patient's diarrhea or other symptom attributed to proton pump inhibitor therapy prescribed for GERD |
The two rows most billers miss are P78.83 and T47.1X5A. A neonate's reflux isn't K21.9, and a PPI side effect needs its own adverse-effect code. Both are clean claims most practices leave on the table.
From Provider Note to Code: The Three-Question GERD Selection Sequence
Selecting the correct GERD ICD-10 code is a three-question decision answered in sequence. Skipping a step is where GERD billing errors start, so work them in order: diagnosis, then esophagitis, then bleeding.
Question 1: Has the provider confirmed a GERD diagnosis?
The note has to name GERD, not imply it. Here's how the documentation routes:
- The note says "GERD" or "gastroesophageal reflux disease," so K21.x is in play. Move to Question 2.
- The note says "heartburn," "reflux symptoms," or "epigastric burning" without naming GERD, so R12 applies until GERD is diagnosed in writing.
- The note says "possible GERD," "probable GERD," or "rule out GERD" in an outpatient setting, so you code the presenting symptom (R12), not K21.9.
The rule underneath all three: the provider has to identify GERD by name. Inferring it from symptoms isn't enough to assign K21.x.
Symptom vs Diagnosis: If the provider documents only "heartburn" without a formal GERD diagnosis, R12 is the correct code, not K21.9. Once GERD is diagnosed in writing, K21.9 replaces R12, and R12 is no longer coded separately.
Question 2: Is esophagitis documented?
With GERD confirmed, esophagitis status picks the code. No esophagitis documented means K21.9. Documented esophagitis, whether the note says "erosive esophagitis," "reflux esophagitis," or "esophagitis due to GERD," moves you to K21.00 or K21.01.
There's a linkage rule that catches coders here. Per the ICD-10-CM Official Guidelines, "with" and "due to" in a code title or the Alphabetic Index both mean "associated with." So a note reading "esophagitis due to GERD" routes to K21.00, even though it never says "GERD with esophagitis."
The Due-To Rule: A note reading "esophagitis due to GERD" triggers K21.00, not K21.9. Per the Official Guidelines, "due to" carries the same weight as "with" in code assignment. Coders scanning only for "GERD with esophagitis" miss the linkage.
Question 3: Is bleeding documented?
No bleeding means K21.00. Bleeding, like hematemesis, GI hemorrhage, or melena attributed to the esophagitis, means K21.01. Missing K21.01 when bleeding is documented weakens necessity for hemostasis (43255), affects the inpatient DRG, and creates a documentation-to-code mismatch that draws audit flags.
Document Bleeding by Name: K21.01 requires the note to state bleeding in the context of esophagitis. A "GI bleed" mentioned without linking it to the esophagitis doesn't trigger K21.01. The note has to connect the two.
The outpatient vs inpatient confirmed-diagnosis rule
Setting changes how an uncertain diagnosis gets coded, and most guides skip this:
|
Setting |
Provider Documentation |
Correct Code |
|---|---|---|
|
Outpatient |
"GERD" (confirmed) |
K21.9 |
|
Outpatient |
"Possible GERD" |
R12 (presenting symptom) |
|
Outpatient |
"Rule out GERD" |
R12 (presenting symptom) |
|
Outpatient |
"Symptoms consistent with GERD" |
R12 (presenting symptom) |
|
Inpatient |
"Probable GERD" |
K21.9 (coded as confirmed) |
|
Inpatient |
"Suspected GERD" |
K21.9 (coded as confirmed) |
Per Section IV.H of the ICD-10-CM Official Guidelines, uncertain diagnoses in outpatient settings code to the presenting symptom. Sections II.H and III.C permit inpatient coding of probable or suspected conditions as confirmed.
Documentation That Survives a GERD Audit: Requirements, Templates, and the LA Grade Table
Most GERD claim denials don't start in the coding department. They start in the provider note. Incomplete documentation before the claim is built is the failure point, and it's the one a biller can't fix after the fact.
What every GERD provider note must include
Seven elements decide whether a GERD claim holds up:
- A GERD diagnosis statement by name, the words "GERD" or "gastroesophageal reflux disease," not a symptom description alone.
- Symptom frequency and duration, like "heartburn 5 to 6 times weekly for 4 months."
- Esophagitis status, present, absent, or not yet evaluated. This single element decides K21.9 vs K21.00 or K21.01.
- Bleeding status whenever esophagitis is confirmed.
- Endoscopy findings, recording the LA Grade (A through D) when inflammation is found, or stating "no esophagitis on visual inspection."
- Treatment response and plan, including drug name, dose, frequency, diet modification, and follow-up.
- Comorbidities that need separate coding, like hiatal hernia, Barrett's, anxiety, or insomnia from nocturnal GERD.
Accurate documentation is a HIPAA requirement under Section I of the Official Guidelines, not a best practice you can skip when the schedule is full.
Three documentation templates
Template 1, Symptomatic GERD Without Endoscopy (Primary Care or Internal Medicine): "Patient presents with heartburn occurring 5-6 times weekly and nocturnal acid regurgitation for 4 months. Conservative management with OTC antacids has provided incomplete relief. No dysphagia, no weight loss, no hematemesis. Clinical assessment: Gastroesophageal reflux disease without esophagitis (K21.9). Plan: Initiate omeprazole 20mg daily, dietary modification counseling provided, elevate head of bed. Follow-up in 8 weeks."
Template 2, GERD Confirmed Post-Endoscopy (Gastroenterology): "EGD performed today. Esophageal mucosa: intact, no erosions, no mucosal injury identified on visual inspection. Biopsies taken from distal esophagus, pathology pending. Gastric mucosa: mild erythema consistent with reflux. Clinical assessment: Gastroesophageal reflux disease without esophagitis (K21.9), pending biopsy confirmation. Plan: Continue pantoprazole 40mg daily, follow up in 2 weeks for biopsy results."
Template 3, Refractory GERD with Esophagitis Confirmed (Gastroenterology): "Patient with 3-year history of GERD, refractory to PPI therapy. EGD today: LA Grade B erosive esophagitis in distal esophagus, no active bleeding. No Barrett's changes on visual inspection, biopsies taken. Clinical assessment: Gastroesophageal reflux disease with esophagitis, without bleeding (K21.00). Plan: Escalate to twice-daily esomeprazole, dietary restriction, consider surgical referral if symptoms persist at 12-week follow-up."
The LA Grade-to-code table
When an endoscopy report grades esophagitis on the Los Angeles classification, that grade maps to code selection and necessity strength:
|
EGD Finding (Los Angeles Classification) |
Code Supported |
Documentation and Necessity Effect |
|---|---|---|
|
Normal mucosa, no breaks |
K21.9 (NERD) |
Supports pH monitoring (91034) workup if symptoms persist |
|
Grade A, mucosal breaks 5 mm or less |
K21.00 or K21.01 |
Grade must be stated in the note, supports PPI continuation |
|
Grade B, breaks larger than 5 mm |
K21.00 or K21.01 |
Supports therapy-escalation documentation |
|
Grade C, breaks spanning folds, under 75% circumference |
K21.00 or K21.01 |
Strengthens necessity for repeat EGD or surgical evaluation |
|
Grade D, 75% circumference or more |
K21.00 or K21.01 |
Strongest support for fundoplication workup (43280) |
The most costly GERD documentation pitfall
Coding K21.9 when the EGD report shows esophagitis is the error that costs the most. The payer reads the procedure note, which confirms esophagitis, against the claim, which says none. The result is a CO-16 denial, a post-payment audit flag, and exposure under the OIG Work Plan, where GI mismatch patterns are a recurring improper-payment area.
EGD-to-Code Alignment: When an endoscopy report confirms esophagitis, the claim has to carry K21.00 or K21.01, never K21.9. Submitting K21.9 after an EGD that found esophagitis is the documentation-to-code mismatch payers and OIG auditors flag first.
Dysphagia documented alongside reflux is an alarm symptom that changes the workup, covered in MedSole's dysphagia ICD-10 guide. The audit patterns above track to the OIG Work Plan.
The GERD CPT Crosswalk: Which Procedures K21.9, K21.00, and K21.01 Actually Justify
The ICD-10 code for GERD doesn't operate in isolation. Every CPT service billed alongside K21.9 has to be justified by the diagnosis, and the diagnosis has to be specific enough to justify the procedure. A vague code can't anchor an expensive scope.
Diagnostic CPT codes linked to K21.x
|
CPT |
Procedure |
Appropriate GERD ICD-10 |
Medical Necessity Threshold |
|---|---|---|---|
|
99213 |
Office visit, established, low complexity |
K21.9, K21.00 |
Symptom documentation plus confirmed GERD diagnosis |
|
99214 |
Office visit, established, moderate complexity |
K21.9, K21.00, K21.01 |
Multiple chronic conditions, moderate-complexity decisions |
|
99215 |
Office visit, established, high complexity |
K21.9, K21.00, K21.01 |
Refractory GERD, comorbidities requiring management |
|
43235 |
Upper endoscopy (EGD), diagnostic |
K21.9, K21.00, K21.01 |
Persistent symptoms, failed PPI therapy, or alarm symptoms |
|
43239 |
EGD with biopsy |
K21.00, K21.01, K22.70 |
Suspected esophagitis or Barrett's on visual inspection |
|
91034 |
Esophageal pH monitoring, 24-hour |
K21.9 |
Refractory GERD, atypical symptoms, pre-surgical evaluation |
|
91010 |
Esophageal manometry |
K21.9, K21.00 |
Dysphagia workup or pre-fundoplication assessment |
|
43280 |
Laparoscopic fundoplication |
K21.9, K21.00 |
Documented failure of conservative and medication therapy |
One accuracy note worth more than it looks: leave the investigational procedures off a standard GERD crosswalk. Codes that most payers treat as investigational generate near-automatic denials, so a focused list of what reimburses beats a long list padded with what doesn't.
Medical Necessity Before Procedure: CPT 43239 (EGD with biopsy) needs a diagnosis that justifies tissue sampling. K21.00 or K22.70 are stronger justifications than K21.9 alone. When an endoscopy finds esophagitis and the claim still shows K21.9, payers flag a procedure-diagnosis mismatch.
The CMS-1500 alignment rule that prevents CO-4 denials
Three fields on the CMS-1500 have to tell one story:
- Box 21 holds the ICD-10 diagnosis, like K21.9 or K21.00.
- Box 24D holds the CPT, like 43235 or 91034.
- Box 24E is the diagnosis pointer linking each 24D service line to the right code in Box 21.
Here's where it breaks. Put 43239 in Box 24D and point it via 24E at K21.9 in Box 21, and the claim says biopsy on one line and no esophagitis on the other. That contradiction draws a CO-4 or CO-16 edit before a human ever reviews it. The second common trigger is 91034 added reflexively, with no documented PPI failure to support it.
CMS-1500 Alignment: Before submission, confirm every CPT in Box 24D is supported by the diagnosis linked in Box 24E. K21.9 pointed at CPT 43239 without a documented esophagitis indication is the most common GERD CO-4 trigger in gastroenterology billing.
The full K21 family detail sits at AAPC. MedSole RCM runs this exact note-to-code-to-CPT alignment check before every gastroenterology claim leaves the building, which is what the outsourced medical billing service handles day to day.
CO-16, CO-50, CO-4: Why GERD Claims Bounce and the Fix for Each
When a GERD claim comes back denied, the code tells you where documentation or coding broke down. Three denial codes account for most GERD rejections, and each one points at a different failure.
The three GERD denial codes
|
Denial Code |
Description |
Root Cause in GERD Claims |
Prevention |
Appeal |
|---|---|---|---|---|
|
CO-16 |
Claim lacks information |
Note doesn't support K21.9, or esophagitis status is absent. EGD report not attached when required |
Pre-submission checklist, GERD stated by name in the assessment |
Corrected claim plus the complete note, citing the documentation that confirms GERD |
|
CO-50 |
Not medically necessary |
Diagnosis doesn't justify the billed CPT, like 43239 billed with K21.9 and no documented indication |
Match the CPT to the most specific code, document an indication for every diagnostic |
Appeal with symptom progression, failed conservative therapy, and clinical rationale |
|
CO-4 |
Service inconsistent with procedure code |
Box 24D CPT misaligned with the Box 21 diagnosis via 24E, like an EGD CPT pointed at K21.9 when esophagitis was found |
Audit 24E pointers pre-submission, use K21.00 when the EGD confirms esophagitis |
Correct and resubmit with the EGD report confirming the finding |
Same-Provider CO-16 Streaks: Three CO-16s on GERD claims from one provider in a month is a documentation-workflow problem, not a coding problem. The assessment line is missing a GERD statement by name or the esophagitis status.
Necessity Anchors: K21.9 alone never justifies advanced diagnostics. Symptom duration, severity, and failed conservative therapy are the medical-necessity anchors every GERD procedure claim needs in writing.
OIG audit triggers
Four patterns put GERD claims on an auditor's radar:
- Coding K21.9 when the procedure report documents esophagitis, the systematic GI mismatch.
- Advanced diagnostics like EGD or pH monitoring with no documented failure of prior conservative therapy.
- Copy-pasted GERD documentation across visits. Identical language every visit triggers Targeted Probe and Educate review.
- Billing K21.01 with no documented bleeding event. Upcoding from K21.00 is a named GI audit target.
Full appeal workflows for each code live in MedSole's denial guides: the CO-16 denial code guide, the CO-50 denial code guide, and the CO-4 denial code guide.
GERD Plus a Second Diagnosis: Pregnancy, Anxiety, Hiatal Hernia, and Nocturnal Insomnia
GERD rarely presents alone. When documented comorbidities are addressed in the encounter, they take their own ICD-10 codes alongside K21.9, and the sequencing rules decide which one leads.
GERD in pregnancy
GERD complicating a pregnancy doesn't lead with the K21 code. The primary code is O99.61-, diseases of the digestive system complicating pregnancy, with the trimester digit: O99.611 for the first trimester, O99.612 for the second, O99.613 for the third, and O99.619 when the trimester isn't documented. K21.9, or K21.00 if esophagitis is confirmed, follows as the secondary code. The Chapter 15 obstetric code sequences first.
A widely republished error routes GERD in pregnancy to O99.89. That code is reserved for conditions not classifiable to a more specific O99 subcategory. GERD is a digestive system disease, so it belongs under O99.61- with the trimester digit, not the catch-all. Reflux ranks among the most common GI complaints in pregnancy, so this one comes up often.
Pregnancy Sequencing: O99.61- with the correct trimester digit leads, and K21.9 follows. Billing K21.9 first on an obstetric encounter generates a sequencing edit from pregnancy-specialized payer systems.
GERD and anxiety
When GERD is the reason for the visit, K21.9 is primary, with F41.1 (generalized anxiety disorder) or F41.0 (panic disorder) as the secondary code. No combination code exists. Code the anxiety only when it's diagnosed and addressed in the plan.
Complexity Upgrade: GERD with a managed anxiety comorbidity (F41.1) can move the E/M level from 99213 to 99214, but the anxiety has to be addressed in the plan. Listing it without managing it justifies nothing.
GERD with hiatal hernia
Sequencing follows the reason for the visit. When the hernia is the cause or the reason for the encounter, K44.9 leads and K21.9 follows. When the patient presents for GERD management and the hernia is contributing, K21.9 leads. Surgical repair (CPT 43281) needs K44.9 as primary.
Hiatal Hernia Sequencing: K44.9 leads only when the hernia itself is the reason for the encounter. When the patient comes in for GERD management and the hernia is incidental, K21.9 leads.
GERD and nocturnal insomnia
Nocturnal reflux that disrupts sleep can carry K21.9 plus G47.01, insomnia due to a medical condition, which is the specific choice when GERD is documented as the cause. G47.00 covers the unspecified version. Don't separately code insomnia mentioned as a symptom only. Code both when both are managed, like a PPI for the reflux and a sleep intervention for the insomnia.
One differential worth flagging: epigastric pain without a confirmed GERD diagnosis routes to R10.13, covered in MedSole's abdominal pain ICD-10 guide. The insomnia co-coding detail is in the insomnia ICD-10 guide, and the transaminitis ICD-10 guide covers a common GI lab finding billed alongside reflux workups.
Is K21.9 Still Current? FY2026, the April 2026 Update, and What FY2027 Changes
Yes. K21.9, K21.00, and K21.01 are active and unchanged under FY2026, covering encounters from October 1, 2025 through September 30, 2026.
Four facts settle the currency question:
The April 1, 2026 release added no new, deleted, or revised diagnosis codes. It revised instructional notes, several Excludes1 to Excludes2 conversions and Code First to Code Also changes, plus index edits, with an updated Official Guidelines edition stamped April 1, 2026. None of it touches the K21 family. The practical implication is combination-coding logic, where conditions previously barred from being reported together may now be reported together when clinically appropriate. It isn't a change to code validity, and there's no invalid-code rejection risk on K21.9 from the April update.
The bleeding distinction has been around longer than most billers think. The K21.00 and K21.01 split dates to the FY2021 update, effective October 1, 2020. That's the point K21.0 stopped being billable on its own.
Looking ahead, the FY2027 files released in June 2026 add 190 new ICD-10-CM diagnosis codes effective October 1, 2026. Review the FY2027 addendum during your annual code-set refresh to confirm the K21 family carries forward before the new cycle starts.
The ICD-9 crosswalk is simpler than some references make it:
|
ICD-9-CM |
Description |
ICD-10-CM |
|---|---|---|
|
530.81 |
Esophageal reflux |
K21.9 |
|
530.11 |
Reflux esophagitis |
K21.00 or K21.01 |
ICD-9 never distinguished bleeding for reflux esophagitis. The K21.00 and K21.01 split is an ICD-10-era refinement, so the crosswalk is two rows, not three. ICD-11, meanwhile, isn't adopted for US HIPAA-covered billing, so K21.x stays mandatory on every US claim.
The current rule set lives on the CMS ICD-10 codes page, and the updated guidelines are in the April 1, 2026 Official Guidelines PDF.
GERD ICD-10 Coding FAQs
What is the ICD-10 code for GERD unspecified?
K21.9 is the ICD-10-CM code for GERD unspecified, gastroesophageal reflux disease confirmed without documented esophagitis. K21.9 is the default GERD code when the provider diagnoses GERD without specifying esophagitis status.
What is the difference between K21.9 and K21.00?
K21.9 is GERD without documented esophagitis. K21.00 is GERD with confirmed esophagitis, without bleeding. The distinction rests on whether the note or endoscopy report documents inflammation of the esophageal lining.
What is the ICD-10 code for GERD with esophagitis?
K21.00 covers GERD with esophagitis without bleeding, and K21.01 applies when esophagitis and bleeding are both documented. The subcode depends on whether the note or EGD report confirms active bleeding.
What ICD-10 code is used for reflux symptoms without a GERD diagnosis?
R12 (heartburn) applies when only symptoms are documented and no GERD diagnosis exists. A note describing acid reflux or heartburn alone, with no formal diagnosis, stays on R12. In outpatient settings, suspected or possible GERD can't be coded K21.9. R12 applies until GERD is diagnosed in writing.
What was the ICD-9 code for GERD?
ICD-9-CM 530.81 (esophageal reflux) crosswalks to K21.9, and 530.11 (reflux esophagitis) crosswalks to K21.00 or K21.01. ICD-9 never separated bleeding, that distinction arrived with ICD-10-CM. ICD-9 codes are invalid for HIPAA-covered billing.
Can GERD and anxiety be coded together?
Yes. When the provider diagnoses and manages both, K21.9 and F41.1 (or F41.0) are reported separately, since no combination code exists. The anxiety has to be addressed in the treatment plan, not merely listed.
What is the ICD-10 code for GERD with hiatal hernia?
Two codes: K21.9 for the GERD and K44.9 for the diaphragmatic hernia. Sequencing follows the encounter reason, K44.9 leads when the hernia is primary, and K21.9 leads when GERD is the reason for the visit.
Is ICD-11 used for GERD billing in the US?
No. ICD-11 isn't adopted for US HIPAA-covered billing, so all US claims stay on ICD-10-CM K21.x. The lineage runs from ICD-9's 530.81 to today's K21.9, but only the ICD-10-CM code is valid on a US claim right now.
The Four Things Every Paid GERD Claim Got Right
Accurate GERD coding is the output of a billing process, not its starting point. The claim fails when documentation, code selection, CPT alignment, or payer validation has a gap, and all four run at the same time.
The four elements
- Provider documentation: a GERD statement by name, esophagitis status, and every billed comorbidity addressed in the plan.
- Code selection: K21.9, K21.00, or K21.01 matching the documented findings exactly, with no inference and no defaults.
- CPT-to-diagnosis alignment: every Box 24D procedure justified by the Box 24E-linked diagnosis.
- Payer validation: the diagnosis, the procedure, and the record all telling the same clinical story.
Match Before Submission: No GERD claim should reach the clearinghouse until the note, the K21 code, and the CPT line tell the same clinical story. Payers adjudicate the match, not the parts.
How MedSole RCM manages GERD billing
MedSole RCM manages the full revenue cycle for gastroenterology, primary care, and internal medicine practices billing GERD encounters across all payer types. The billing fee is 2.99% of collections, with no setup fees and no long-term contracts. The clean claim rate on GERD encounters is 99%. For practices that need enrollment before billing, MedSole RCM credentials providers at $99 per payer, $1,980 for a 20-payer panel, against an industry range of $150 to $300 per payer. The team monitors every ICD-10-CM release, including mid-year instructional updates like April 1, 2026, so claims are never coded against a stale rule set. The billing side is detailed on the outsourced medical billing services page, and credentialing is covered under provider enrollment and credentialing services.
The GERD ICD-10 decision in four lines
- Use K21.9 when GERD is confirmed and esophagitis isn't documented.
- Use K21.00 when GERD is confirmed and esophagitis is documented without bleeding.
- Use K21.01 when GERD is confirmed and both esophagitis and bleeding are documented.
- Use R12 when only heartburn symptoms are documented and GERD hasn't been diagnosed.
Get those four lines right and most GERD denials never reach your desk. The code is the easy part once the documentation and the workflow behind it hold up.